




A 7-year-old boy with no relevant past history was evaluated by the dermatologist at the emergency department of our hospital regarding the presence of several asymptomatic spots on his hands. The lesions had appeared after the boy had been playing with worms in the school playground and were resistant to soap and water. His mother said that some children who had been playing with him had similar spots, although to a lesser extent.
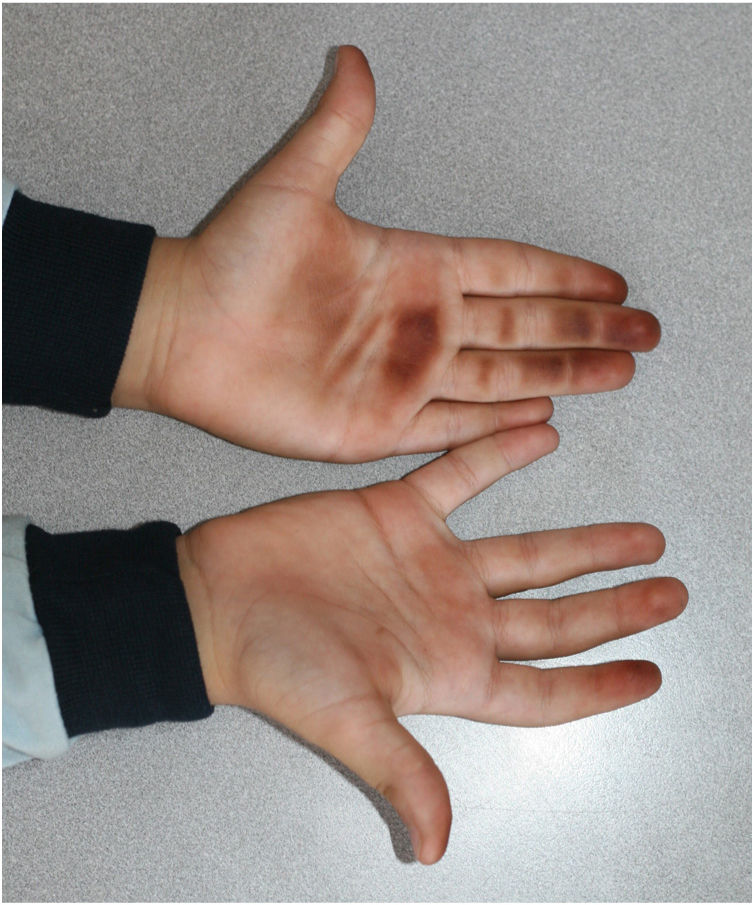
Physical ExaminationPhysical examination showed poorly defined reddish-brown macules on the boy's palms and on some fingers, in particular the first and second fingers of the right hand (Figs. 1 and 2).

Dermoscopy showed pigmentation with a ridge pattern and sparing of the acrosyringeal apertures.
HistopathologyHistologic examination of a punch biopsy specimen showed no relevant findings in the dermis or epidermis, or pigmented substances in the stratum corneum.
Additional TestsThe mycobacterial culture was negative.
What Is Your Diagnosis?
DiagnosisExogenous pigmentation induced by the handling of millipedes.
Clinical Course and TreatmentThe boy was shown some photographs of worms he might have been playing with in the school playground and clearly identified the Tanzanian red-legged millipede. One week later the lesions showed clear clinical improvement without treatment.
CommentEpibolus pulchripes, otherwise known as the Tanzanian red-legged millipede, is a member of the Diplopoda class. Although it inhabits tropical and subtropical areas of West Africa, its presence in southern and eastern Spain could be related to migratory phenomena or accidental introduction with displacement of native millipede species.
When the arthropod feels threatened, it curls up and releases substances rich in cyanide and quinones through pores in its exoskeleton. Contact with cyanide can cause inflammation, itching, or stinging, as well as vesiculation or ulceration in the event of prolonged contact. Quinone compounds secreted as chemical defense mechanisms cause hyperpigmentation of the skin and mucous membranes.1,2 The pigmented spots on the palms of the boy in our case would have been caused by quinone secreted by the millipede when crushed.
Reports of similar cases to ours have described an asymptomatic reddish-brown or black spot in the contact area after accidental crushing of other species of millipedes and even spots reproducing the shape of the millipede.3 The most common locations affected are the toes and neck, although the mouth may sometimes be involved. Eye contact can cause conjunctivitis or corneal ulcers.1
Diagnosis is usually established clinically with a careful history. Manifestations can sometimes mimic cutaneous manifestations of systemic diseases, or even acute arterial occlusion.4,5
The ridge pattern on dermoscopy is common. When observed, acral melanoma, which manifests as a brown-black spot, must be ruled out.2
Other entities in the differential diagnosis include metabolic disorders, infections such as tinea nigra, exposure to other exogenous substances such as henna, silver nitrate, or potassium permanganate, and contact with certain plants. All these diagnoses were ruled out in our case by clinical history and complementary tests.
Lesions heal spontaneously and do not require treatment, although topical alcohols may be used. Itching or irritation can be treated with topical corticosteroids.1,2,5


