





The common feature of these 3 pigmented lesions (Fig. 1), apart from occurring in men, their localization on the back, and their uncertain history (probably because of their site), is that they are lesions that are regressing. This is easy to identify on dermoscopy because of the presence of gray-blue granules or globules with a variable degree of confluence1–3; these can be seen on the left side of the image of the first lesion (Fig. 2), in the upper part of the image of the second lesion (Fig. 3), and on the right side of the image of the third lesion (Fig. 4). The histopathological explanation of this gray-blue granule-globule pattern is the presence of melanophages.
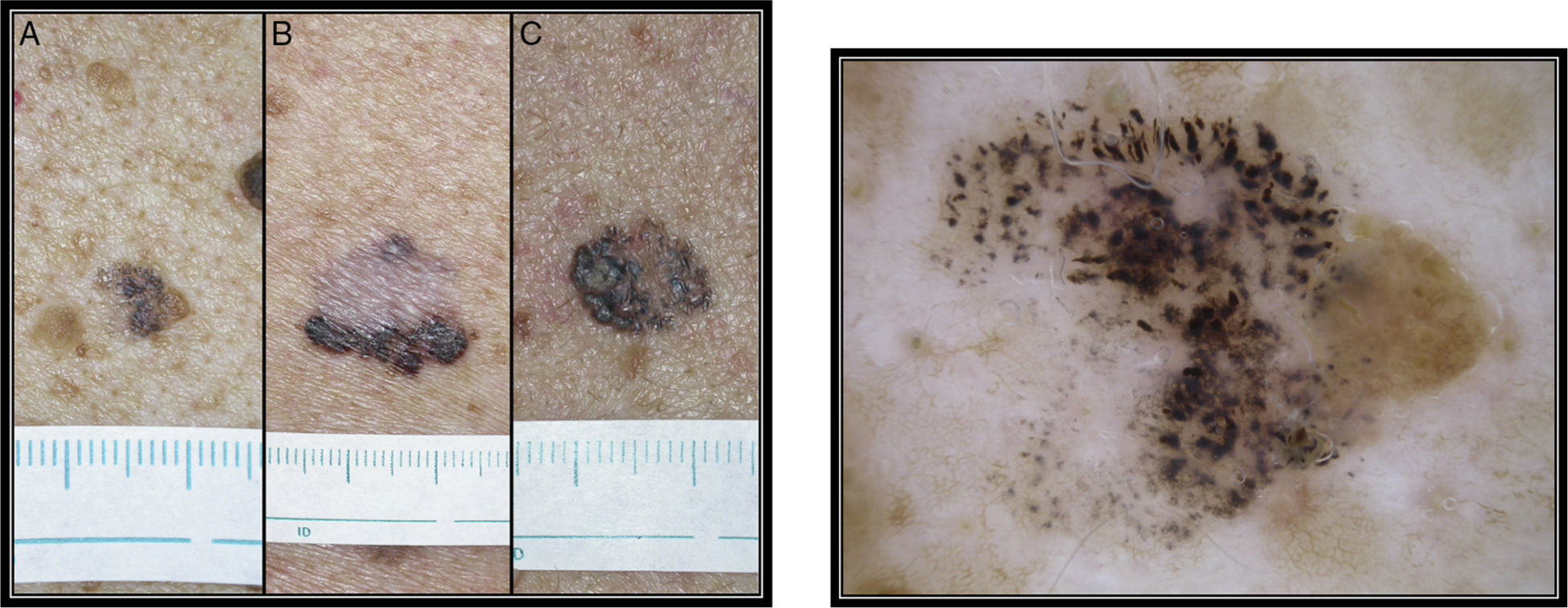
Three pigmented lesions, present for an unknown time, situated on the backs of 3 patients. A, In a 55-year-old man (clinical image in Fig. 1A and dermoscopy in Fig. 2). B, In a 90-year-old man (clinical image in Fig. 1B and dermoscopy in Fig. 3). And C, In a 39-year-old man (clinical image in Fig. 1C and dermoscopy in Fig. 4).
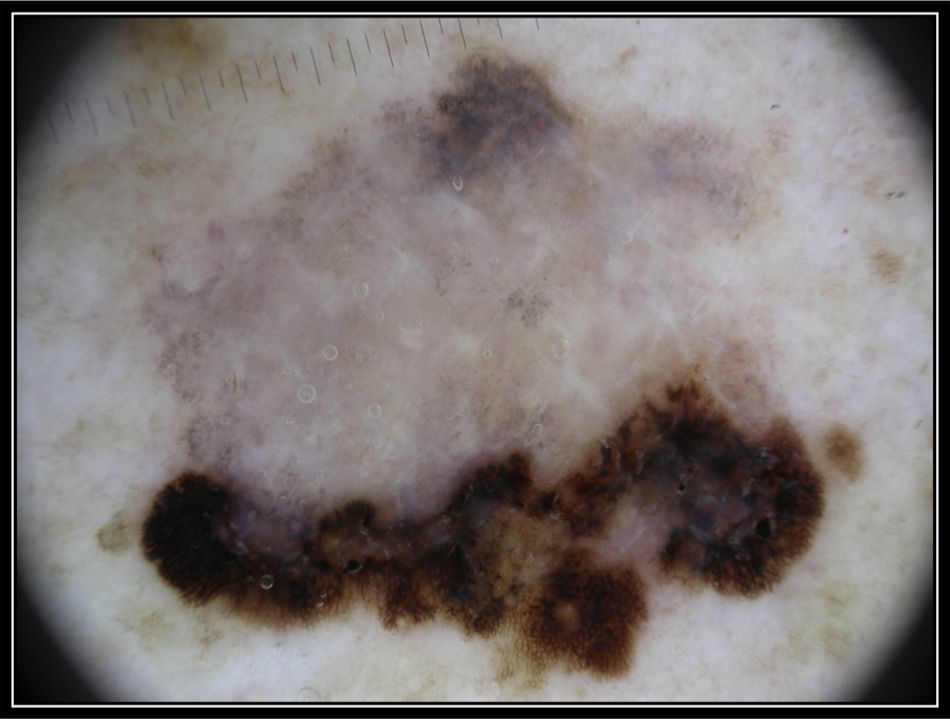
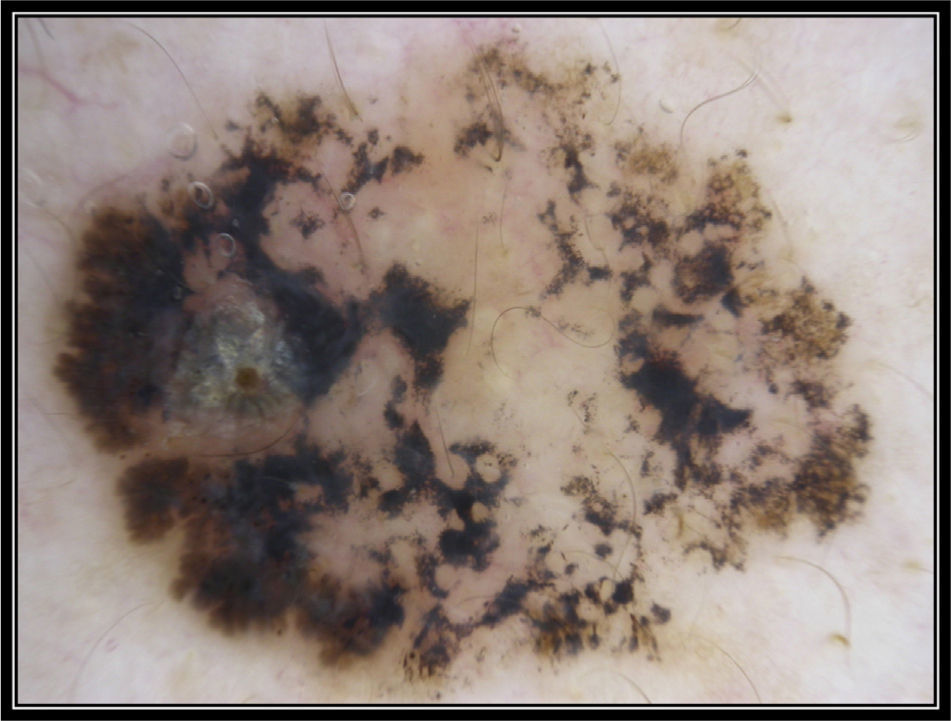
When investigating a lesion that is in regression, the most important issue is to determine the nature of the lesion. Dermoscopy can be a useful tool. Looking at the dermoscopy images of the lesions, we can identify the residual areas that are in regression: the right side of lesion in the first case, the inferior part in the second case, and the left side in the third case. In the first case (Fig. 2), we can see fissures and ridges, crypts, and comedo-like openings, which are characteristic dermoscopic structures of seborrheic keratoses. In the second case (Fig. 3), an atypical pigment network is present, associated with pseudopods, atypical dots and globules, a pigmented structureless area in the superior part, and areas of mixed regression; together, these dermoscopic structures are very suggestive of superficial spreading melanoma. Finally, in the third case (Fig. 4) we can see a number of brown-colored bulbous projections situated at the periphery of the lesion. These structures are reminiscent of the lobed leaves of certain plants and they are known as maple leaf-like areas; they are highly characteristic of pigmented basal cell carcinoma.1
Thus the dermoscopic diagnosis in the first patient would be regressing seborrheic keratosis or, if preferred, an intermediate stage in the transformation of a seborrheic keratosis into lichenoid keratosis.2,3 The diagnosis in the second patient would be regressing superficial spreading melanoma and, in the third case, regressing basal cell carcinoma. The 3 diagnoses were confirmed by the pathologist after biopsy of the first lesion and excision of the other two.
Please cite this article as: Zaballos-Diego P. Vestigios. Actas Dermosifiliogr. 2014;105:791–792.


