



Pulsed dye and carbon dioxide lasers have been applied in dermatofibroma with clinical improvement. We treated 23 dermatofibromas two times at a 4-week interval with Q-Switched alexandrite laser 755 nm (7.5 J/cm2, 3 mm, 50 ms). V Beam pulsed dye laser with a wavelength of 595 nm was used for the residual erythema (10-11 J/cm2, 7 mm, 1.5 ms). A partial attenuation of brown colour was observed in 9 patients and complete disappearance of brown colour in 14 patients. Patient satisfaction was very high. Fifteen patients felt a decrease in hardening of dermatofibroma after treatment. A pigment network in dermoscopy was observed in all patients before treatment and no one after treatment. A combined treatment using both V Beam pulsed dye laser and Q-Switched alexandrite laser may be a therapeutic option to reduce the aesthetic effect of dermatofibroma with a high patient satisfaction and good cosmetic outcomes.
El uso de los láseres de colorante pulsado (pulse dye laser [PDL]) y de dióxido de carbono (CO2) para el tratamiento de los dermatofibromas (DF) ha demostrado tener buenos resultados clínicos. Un total de 23 DF fueron tratados en dos sesiones con el láser de alejandrita Q-Switched de 755 nm (7,5 J/cm2, 3 mm, 50 ms), dejando entre cada sesión un intervalo de 4 semanas. Para el eritema residual se utilizó el láser V Beam PDL con una longitud de onda de 595 nm (10-11 J/cm2, 7 mm, 1,5 ms). En 9 de las pacientes se observó una atenuación parcialde la coloración marrón y en 14 de ellas una desaparición completa de la misma. Las pacientes refirieron un grado elevado de satisfacción después de haber realizado el tratamiento. Así mismo, 15 de las pacientes notaron una disminución en el endurecimiento de los DF. En el examen dermatoscópico previo al tratamiento, en todos los DF se observó la presencia de una red de pigmento. Esta red de pigmento desapareció en todos los casos tras la aplicación del láser. La combinación del láser V Beam PDL y del láser de alejandrita Q-Switched en los DF constituye una alternativa terapéutica adecuada que, además de buenos resultados cosméticos, ha conseguido un elevado grado de satisfacción por parte de los pacientes.
Dermatofibroma (DF) is a benign skin tumor of fibroblastic origin. Lesions are often located on the upper and lower limbs of adult patients. Treatment of DF is only necessary when symptomatic or for esthetic reasons.1 The aim of this study is to report our experience treating DF with a combination of Q-Switched alexandrite laser and V Beam pulsed dye laser.
MethodsInclusion criteria were the clinical and dermatoscopic findings of the DF (dimpling, peripheral pigmentation, and white central patch), more than a year since onset, age over 18 years, and not having undergone prior treatment in the past 3 months. DF that fulfilled typical clinical and dermatoscopic criteria were chosen and a total of 23 cases were included. All patients gave signed informed consent in order to take part in the study.
The Q-Switched alexandrite laser with a wavelength of 755 nm (Alex Lazr, Syneron Candela, Boston, MA, USA) was used. The parameters used were a fluence of 7.5 J/cm2, a spot size of 3 mm, and a pulse duration of 50 ms. Local anesthetic was not required. Each lesion was treated in 2 sessions, with an interval of 4 weeks between sessions. Post-treatment care included application of petrolatum cream twice daily for a week. The V Beam pulsed dye laser (Alex Lazr, Syneron Candela, Boston, MA, USA), with a wavelength of 595 nm was used to improve residual erythema secondary to application of the Q-Switched alexandrite laser. The parameters used were a fluence of 10-11 J/cm2, a spot size of 7 mm, and a pulse duration of 1.5 ms.
Patients were followed up for 2 months. Clinical and dermatoscopic images of the DF were taken before and after treatment. Similar lighting, the same camera setup, the same dermatoscope (Handyscope for Ipod touch, Fotofinder Systems GmbH, Bad Birnbach, Germany), and the same image-processing technique were used to ensure that the images were comparable. Three different dermatologists evaluated the effectiveness and safety of the treatment (comparison of interobserver agreement) by assessing changes in color, degree of hardening, patient satisfaction (0-10 points), and adverse effects observed before and after treatment.
ResultsAll patients were women aged between 25 and 67 years (mean, 51.2 years). Time since onset of the DF varied between 2 and 40 years (mean, 15 years). Fourteen patients had phototype III on the Fitzpatrick scale, 8 had phototype II, and 1 patient had phototype I. Twenty-one of the DF were located on the lower limbs and only 2 were located on the arms. None of the patients reported associated symptoms before or after treatment. Partial clearance of the brown color was observed in 9 DF, whereas complete clearance was observed in 14. Patients reported a high degree of satisfaction (mean, 8 points). Furthermore, after treatment, 15 patients reported a reduction in the degree of hardening of the DF (Fig. 1A and 1B). Dermatoscopy before application of the laser revealed pigmentation in all the DF. This pigmentation disappeared in all cases after treatment Fig. 1C and 1D). Before application of the laser, 10 of the DF revealed diverse structures with a vascular appearance. After laser treatment, however, these structures were observed in 18 of the DF. The white central patch was present in all cases of DF, both before and after treatment. Erythema (reddish coloring of the post-laser lesion) was the most frequent adverse effect and was observed in 14 of the DF. The erythema disappeared after application of the V Beam pulsed dye laser (595 nm; 10-11 J/cm2; 7 mm; 1,5 ms) Fig. 1E). Only one of the patients (with phototype I on the Fitzpatrick scale) showed residual hypopigmentation.
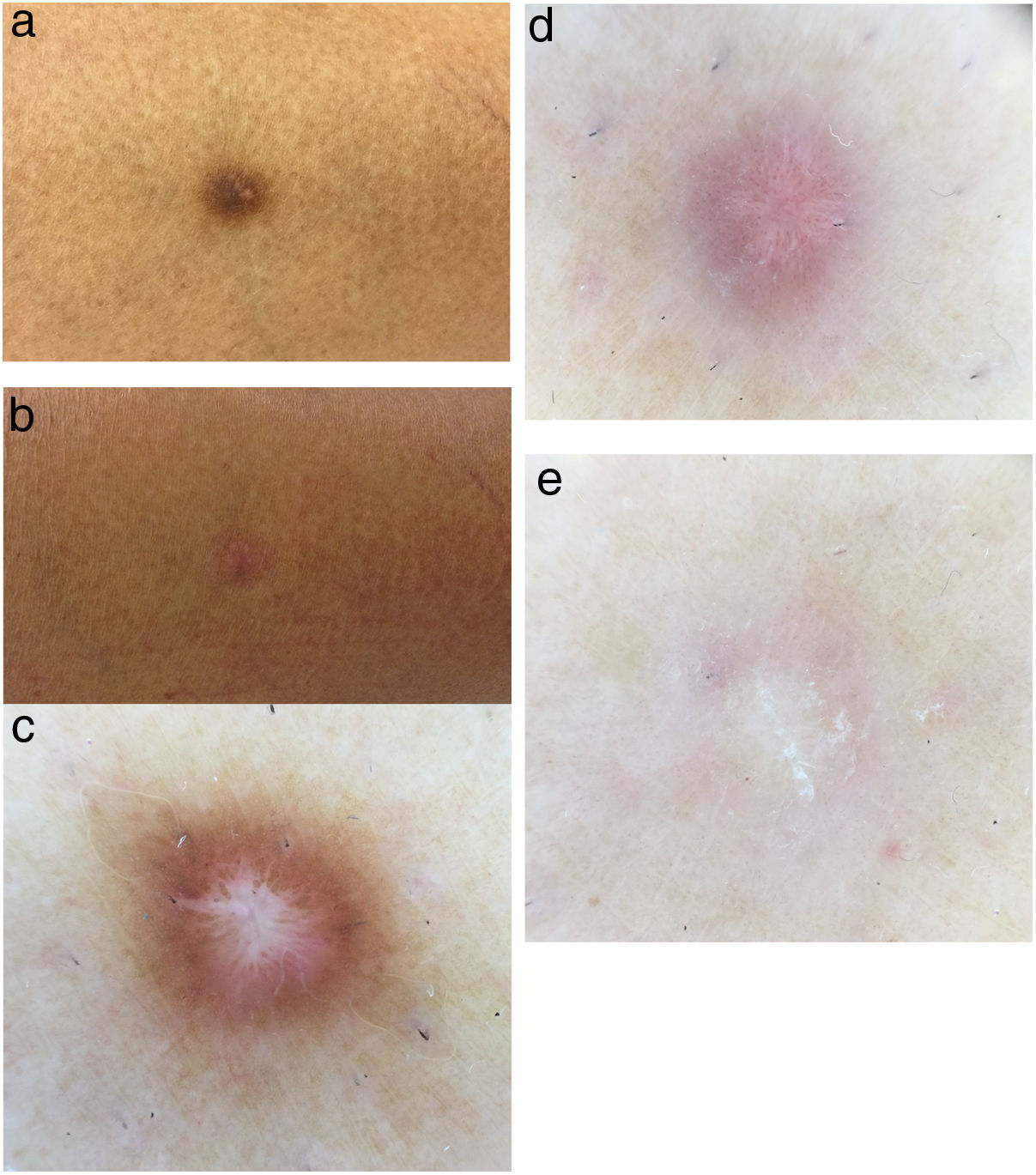
A, Dermatofibroma before treatment; B, Dermatofibroma after treatment; C, Before treatment, the dermatofibroma shows peripheral pigmentation accompanied by a white central patch; D, After treatment with the Q-Switched alexandrite laser with a wavelength of 755 nm, dermatoscopy of the dermatofibroma shows vascular structures and a white central patch; E, After treatment with the 595-nm pulsed dye laser, dermatoscopy of the dermatofibroma shows a white central patch.
Surgical excision of DF is generally considered to be a cure and presents local recurrence of less than 2%. Surgery, however, may produce unwanted scars. Nonsurgical therapeutic alternatives described include cryotherapy and intralesional injection of corticosteroids. This last treatment is of limited and variable efficacy, and may cause adverse effects in some cases.1 No standard approach exists to the treatment of DF and management of these lesions continues to be a therapeutic challenge.
Different types of laser have been used to treat DF. Pulsed dye laser has been shown to provide clinical improvement in these lesions and to have adequate cosmetic results.1,2 Wang and Lee1 reported 20 DF treated in 3 sessions with pulsed dye laser (600 nm; 7 J/cm2; 7 mm; 1,5 ms). In terms of reduction of lesion size, 15 of the 20 DF (75%) presented a complete clinical response, whereas 5 (25%) showed a partial response. In terms of improvement in coloring, 12 of the 20 DF (60%) presented a complete and 8 (40%) showed a partial response. The authors of that study concluded that pulsed dye laser provided a better esthetic result than surgical excision.1
Wang and Lee1 reported 22 DF treated in between 1 and 3 sessions with pulsed dye laser (595 nm; 11 J/cm2; 7 mm; 2 ms). Six of these cases showed clinical improvement of over 75%, 6 showed an improvement of between 50% and 75%, 8 showed improvement of between 25% and 50%, and 2 showed improvement of less than 25%. Dermatoscopy revealed changes in all those cases of DF. Full clearance of pigmentation was found in 12 of the DF (54%) and pigmentation was merely reduced in 9 (40%). Postinflammatory hyperpigmentation or hypopigmentation was the only adverse effect reported and this resolved spontaneously 6 months after treatment. Because the target of the pulsed dye laser is oxyhemoglobin and not melanin, the mechanism of action in DF is not fully understood.
Wang et al3 reported good results after treating DF located on the thigh with a CO2 laser (450-500 nm; 1-4 passes; 3-5 mm; 500-600 ms) in 3 sessions, with an interval of 5 weeks between each session; a topical corticosteroid was also used in that study. That treatment produced complete flattening of the lesion and disappearance of the pruritus. Minimal postinflammatory hyperpigmentation was also observed.
The use of CO2 laser in multiple facial DF has also been described; however, details of the parameters used were not provided.4
While preliminary, our study has shown that the Q-Switched alexandrite laser is an effective and safe therapeutic alternative for the treatment of DF. Patients also reported a high degree of satisfaction, which is closely related to the complete or partial disappearance of the brown color of the lesions. Most patients choose a nonsurgical solution, which avoids the risk of scarring and a poor esthetic result.
DF are characterized clinically by considerable hyperpigmentation and treating the visible surface pigment using a Q-Switched alexandrite laser is therefore a logical approach. The residual erythema observed in 14 of the DF 2 months after the last laser session was reduced notably after application of the V Beam pulsed dye laser. We therefore believe that the combination of the V Beam pulsed dye laser and the Q-Switched alexandrite laser will improve the final cosmetic result in DF. Furthermore, 65% of patients reported a reduction in the degree of hardening of the DF.
To our knowledge, the use of the Q-Switched alexandrite laser as a therapeutic option in DF has not been reported to date. The limitations of this study include the small number of cases, the lack of histologic findings, the short follow-up period, measurement of a subjective variable such as degree of hardening of the DF, and the lack of another comparative treatment. More clinical studies will be required to evaluate the efficacy, safety, and cosmetic results of the combination of Q-Switched alexandrite laser and pulsed dye laser in DF.Although the treatment of choice in DF is surgical excision, this may produce unwanted scarring. We therefore believe that the combination of the Q-Switched alexandrite laser and the V Beam pulsed dye laser will be a valid therapeutic alternative for reducing the least esthetic characteristics of DF.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Imbernón-Moya A, Beleña-Cárdenas M, Ruiz-Rodríguez R, Sánchez-Carpintero I. Estudio prospectivo de la combinación de láser de alejandrita Q-Switched de 755 nm y el láser V Beam de colorante pulsado de 595 nm en dermatofibromas. Actas Dermosifiliogr. 2020;111:257–260.


