
Phototherapy is one of the main therapeutic options in atopic dermatitis (AD), of which narrowband UV-B (NB-UVB: 311 [2] nm) is one of the most effective modalities.1–3 We report the results of a retrospective observational study carried out over 1 year, the objective of which was to evaluate the effectiveness of this treatment using severity and quality of life scales.
The study included patients with AD who had been referred from dermatology consultations to the phototherapy unit to be treated with NB-UVB. The exclusion criterion, beyond those criteria inherent to phototherapy, was age below 18 years.
A UV-7002® booth (Waldmann, Schwenningen, Germany) with 21 F79/120W-TL01 tubes (311 nm) and 21 UVA tubes was used. Patients entered the booth with dark UV-protection glasses and men wore genital protection.
Sociodemographic data, Fitzpatrick skin type, and minimal erythema dose (MED) in J/cm2 to calculate the initial dose were recorded. Treatment was administered 3 days per week, with weekly dermatologic check-ups.
Prior treatments associated with the phototherapy cycle were recorded, together with the characteristics of the NB-UVB treatment (number of sessions and start, end, and total dose in J/cm2).
We used the Eczema Area and Severity Index (EASI) and Skindex-29 to measure the severity of the disease and quality of life of the patients, respectively.
Adverse effects (AE; erythema and pruritus) were defined as mild (asymptomatic), moderate (erythema and transitory pruritus < 24 h), and severe (erythema and pruritus > 24 h).4 Pruritus was measured at the beginning and end of treatment using a visual analog scale (VAS).5
Goodness of fit of the variables was determined using the Kolmogorov-Smirnov test. Statistical inference was performed using the Mann-Whitney U, Wilcoxon, or ANOVA tests, as applicable. Values of P < .05 were considered to be statistically significant. The statistics program used was SPSS v.25.0.
All aspects followed routine clinical practice. The data were collected from the patients’ phototherapy and electronic medical records. The study was approved by the research ethics committee of our autonomous region.
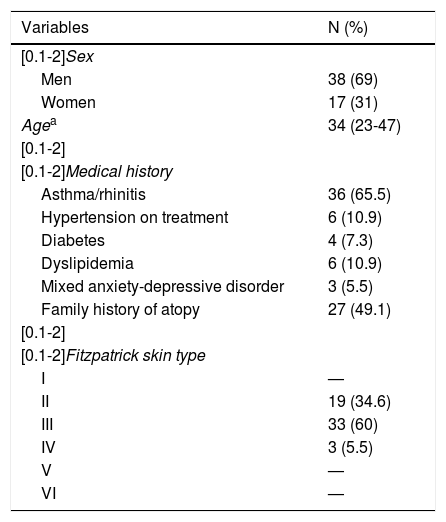
A total of 55 patients were enrolled, 38 of whom were men, with a mean age of 34 years (23-47 years) (Table 1). Sixty percent of patients had Fitzpatrick skin type III.
Descriptive Analysis of the Study Population.
| Variables | N (%) |
|---|---|
| [0.1-2]Sex | |
| Men | 38 (69) |
| Women | 17 (31) |
| Agea | 34 (23-47) |
| [0.1-2] | |
| [0.1-2]Medical history | |
| Asthma/rhinitis | 36 (65.5) |
| Hypertension on treatment | 6 (10.9) |
| Diabetes | 4 (7.3) |
| Dyslipidemia | 6 (10.9) |
| Mixed anxiety-depressive disorder | 3 (5.5) |
| Family history of atopy | 27 (49.1) |
| [0.1-2] | |
| [0.1-2]Fitzpatrick skin type | |
| I | — |
| II | 19 (34.6) |
| III | 33 (60) |
| IV | 3 (5.5) |
| V | — |
| VI | — |
The MED was pathological in 12 patients. And the median number of sessions was 29 (21-38). The median of the initial, final, and end doses were 0.25 J/cm2 (0.21-0.35), 1.44 J/cm2 (0.86-1.95), and 25.39 J/cm2 (9.52-39.11), respectively.
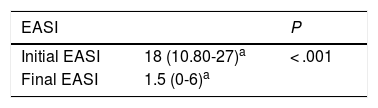
The difference between the initial and final EASI score was statistically significant (P < .001) (Table 2). An EASI 50 was achieved in 44 patients (80%) and clearance was achieved in 23. The final EASI score was not determined in 3 patients because they abandoned treatment for personal reasons.
Analysis of the EASI and Skindex-29 Scores.
| Skindex-29 Subscore | Mediana | P |
|---|---|---|
| [0.1-3]Emotional | ||
| Baseline | 57.5 (40-70) | |
| Final | 25 (18.75-47.50) | P < .001 |
| [0.1-3] | ||
| [0.1-3]Functional | ||
| Baseline | 43.74 (31.25-52.07) | |
| Final | 20.83 (3.12-30.20) | P < .001 |
| [0.1-3]Overall | ||
| Baseline | 50.86 (36.20-62.02) | |
| Final | 25 (12.06-37.06) | P < .001 |
| [0.1-3]Symptomatic | ||
| Baseline | 53.57 (39.28-64.28) | |
| Final | 25 (16.07-41.06) | P < .001 |
The difference between the initial and final Skindex-29 score, calculated in 12 patients, was statistically significant (P < .001) (Table 2).
Eight patients did not respond to treatment: 7 required immunosuppressant treatment prior to the phototherapy cycle (5 oral corticosteroids, 1 azathioprine, and 1 cyclosporin). The patients treated with azathioprine or cyclosporin showed a significantly worse response (P = .005).
In 47 patients, the phototherapy was combined with oral corticosteroids (12 patients), topical corticosteroids (15 patients) or UVA (20 patients), with a median initial EASI score of 27.10 (22.42-42.50), 18 (7.20-25), and 16.40 (10.20-23.55), respectively, higher than in the group treated with phototherapy alone (initial EASI score: 12 [7.17-19.25]). The difference between the final EASI score for the 2 groups was not statistically significant (P = .331).
With regard to AEs, 8 patients presented erythema (mild in 4 patients and moderate in the rest), and 1 patient presented a polymorphous light eruption. A 50% reduction in the initial EASI score (EASI 50) was achieved in 7 patients. It was not necessary to suspend treatment due to the AEs.
The reduction in the EASI score was statistically significant (P < .001), with a greater percentage than previously published.6
Although the Skindex-29 was calculated in only 12 patients, the reduction in the symptomatic and functional subscores was above 40%, which, like other authors,7 we believe to be the subscores that most affect daily activity.
The most severe patients were those who received combined treatment, although this did not significantly improve their response. We found no other studies that support this result. The AEs did not have a negative effect on the therapeutic response; we found no bibliographic references in this regard.
Nine patients presented AE that did not require suspension of the treatment.6,8 We did not assess whether the pruritus associated with the atopic dermatitis may have affected the therapeutic response, unlike published studies in patients with psoriasis.9
We did not find the pathologic MED in 12 patients to be linked to concomitant medications nor to an increase in adverse reactions, given the modification of the protocol based it.10
The limitation of this study is the fact that it is a retrospective and single-center study. One of its strengths is the sample size, which is larger than that of other studies.
Please cite this article as: Pérez Feal P, Estany Gestal A, Rodríguez-Tubío Dapena S, Rodríguez Granados MT. Fototerapia ultravioleta B de banda estrecha en pacientes con dermatitis atópica: estudio en un hospital de tercer nivel: estudio retrospectivo y observacional. Actas Dermosifiliogr. 2020. https://doi.org/10.1016/j.ad.2019.10.005


