


Giant vascular eccrine spiradenoma is a rare variant of eccrine spiradenoma characterized by its size (> 2cm diameter) and high vascularity, a feature that often leads to it being confused with tumors of vascular origin. We present a case of this rare tumor.
A 54-year-old woman presented with a tumor that had been present for years, measuring 2.3×2×2.6cm, located on the medial aspect of the left arm (Fig. 1A). The tumor was a reddish, dome-shaped lesion, ulcerated on one side, and hard to palpation. The patient attended because the mass had increased in size and at some point there had been a small amount of bleeding. Magnetic resonance imaging (MRI) was performed to investigate the clinical suspicion of a tumor of vascular origin. The different projections (sagittal plane on T2; transverse plane on T1, T2, FFE T2, and STIR) showed a mass located in the subcutaneous cellular tissue, which was presumed to be of vascular origin given that it was described as being dependent on and draining into the basilic vein (Fig. 1B). The lesion was mottled and multilobulated. There was no intramuscular component and the surrounding tissues were unchanged. On the basis of these findings, we proceeded to surgical excision and histopathological study. The tumor, situated in the mid-dermis and deep dermis, was composed of several well-demarcated lobules separated by fine bands of fibrous tissue with abundant dilated and congested vascular structures (Fig. 2). The lobules were arranged in aggregates of cells, some with a basaloid appearance and others with a larger, clearer cytoplasm, arranged in cords, trabeculae, and solid nests with duct-like structures. On immunohistochemical study, most of the cells expressed pan cytokeratins, and the luminal cells expressed carcinoembryonic antigen (CEA).
.")
.")
Spiradenomas are rare benign tumors derived from the inferior portion of eccrine sweat ducts, and they usually develop on the head, neck, trunk, and, less often, the limbs. Their main clinical characteristic is that they are generally painful. Typically, spiradenomas present in patients aged between 15 and 35 years of age and they are usually solitary, although different clinical presentations have been described.
In 1986, Cotton et al1 described two cases of eccrine spiradenoma that they classified as giant vascular type due to their large size and high vascularity. Since then, to the best of our knowledge, 12 further cases have been described (Table 1). The first description referred to a classic spiradenoma, measuring over the established 2cm diameter, with the most salient feature being its high vascularity. Many authors have described this high vascularity as the result of a stromal involution process due to ageing of the lesion.7,9 This concept is defended by some authors,9 but in our case the information supplied by MRI supported the existence of a tributary vessel. This vessel made it easy to mistake the mass for a vascular tumor, and it would also have promoted tumor growth. The most notable feature in this case was the finding of an afferent vessel to the tumor with drainage into the basilic vein, leading the radiologist to suspect a slow flow vascular malformation. Similarly, the marked vascularization of these tumors means that most eccrine spiradenomas are clinically diagnosed as benign or malignant neoplasms of vascular origin. The most important differential diagnoses are angiosarcoma, which expresses endothelial markers such as CD31 and CD34, and chronic expansive hematoma, which presents as an encapsulated tumor filled with blood and neovasculature.
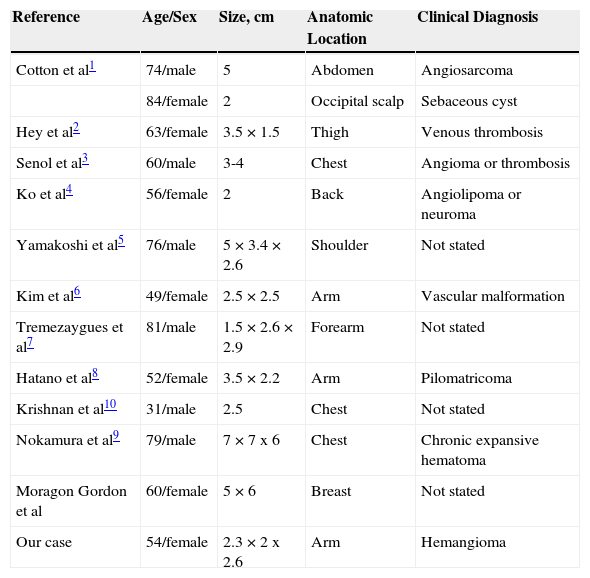
Clinical Characteristics of Giant Vascular Eccrine Spiradenomas.
| Reference | Age/Sex | Size, cm | Anatomic Location | Clinical Diagnosis |
|---|---|---|---|---|
| Cotton et al1 | 74/male | 5 | Abdomen | Angiosarcoma |
| 84/female | 2 | Occipital scalp | Sebaceous cyst | |
| Hey et al2 | 63/female | 3.5×1.5 | Thigh | Venous thrombosis |
| Senol et al3 | 60/male | 3-4 | Chest | Angioma or thrombosis |
| Ko et al4 | 56/female | 2 | Back | Angiolipoma or neuroma |
| Yamakoshi et al5 | 76/male | 5×3.4×2.6 | Shoulder | Not stated |
| Kim et al6 | 49/female | 2.5×2.5 | Arm | Vascular malformation |
| Tremezaygues et al7 | 81/male | 1.5×2.6×2.9 | Forearm | Not stated |
| Hatano et al8 | 52/female | 3.5×2.2 | Arm | Pilomatricoma |
| Krishnan et al10 | 31/male | 2.5 | Chest | Not stated |
| Nokamura et al9 | 79/male | 7×7x6 | Chest | Chronic expansive hematoma |
| Moragon Gordon et al | 60/female | 5×6 | Breast | Not stated |
| Our case | 54/female | 2.3×2x2.6 | Arm | Hemangioma |
What was interesting about this case, apart from the rarity of the condition, was the ease with which a giant vascular eccrine spiradenoma could be mistaken for a lesion of vascular origin.
Please cite this article as: Jorquera Barquero E, Lara Bohórquez C, de Alba Rioja I. Espiradenoma ecrino vascular gigante. Actas Dermosifiliogr. 2015;106:850–852.


