


Cutaneous fibrolipomatous hamartoma (CFH) is characterized by the presence of lobules of mature adipose tissue surrounded by fibrous septa in the mid-to-deep dermis. In the literature, this entity has several different names, although the most widely used is precalcaneal congenital fibrolipomatous hamartoma.1
Clinically, the condition presents as a soft, flesh-colored, asymptomatic, solitary mass. It is generally bilateral and symmetrical and located on the inner part of the plantar aspect of the heel, or precalcaneal region. Cases of unilateral involvement have been reported,2,3 and, although this is a congenital lesion, it is sometimes first noticed years after birth.3 Most cases are sporadic, although the possibility of autosomal dominant or X-linked inheritance has been postulated.1,3,4
The diagnosis is mainly clinical. However, in doubtful cases, such as unilateral involvement or uncharacteristic sites, biopsy is usually the approach taken. The differential diagnosis is with infantile hemangioma, congenital hemangioma, vascular malformations, lipoma, and neurofibroma. Skin imaging with high-frequency ultrasound can facilitate the differential diagnosis and confirm the clinical suspicion, thus obviating the need for invasive diagnostic tests.
Case DescriptionWe present a clinical and ultrasound image of CFH in a 5-month-old girl with no personal history of interest. Clinically, the image shows an asymptomatic flesh-colored mass that was soft in consistency. The lesion had been present since birth and had grown in proportion with the patient. No similar change was observed on the contralateral foot (Fig. 1). The patient was an only child, and the parents did not have similar abnormalities.

The ultrasound image confirmed the clinical suspicion and made it possible to rule out differential diagnoses (Fig. 2). We did not observe any masses or tumors or clusters of anechoic channels with or without internal flow. The lacunae did not disappear on compression of the skin by the transducer. Doppler mode did not reveal a signal in the interior or periphery of the lesion.
 of fibrolipomatous hamartoma. A, Longitudinal plane (A). B, Transversal plane (B). Note the thickening of the dermis and hypodermis at the expense of hypoechoic islands with fatty echogenicity intermingled between hyperechoic lines in the deep dermis, which extend to the subcutaneous cellular tissue.")
Ultrasound image (18MHz) of fibrolipomatous hamartoma. A, Longitudinal plane (A). B, Transversal plane (B). Note the thickening of the dermis and hypodermis at the expense of hypoechoic islands with fatty echogenicity intermingled between hyperechoic lines in the deep dermis, which extend to the subcutaneous cellular tissue.
The parents were informed that the lesion was benign and did not require treatment. The lesion was to be reviewed only in the case of changes or onset of symptoms.
DiscussionSkin imaging with high-frequency ultrasound is increasingly used in childhood dermatologic diseases. The differential diagnosis of tumors is one of its main applications. Unlike tumors, hamartomas appear as thickening of the dermis and/or subcutaneous cellular tissue and not as masses. The echogenicity of a hamartoma depends on the most abundant element. In the case of CFH, the reticular dermis thickens owing to the presence of islands of fatty tissue between collagen fibers that can extend to the hypodermis. Ultrasound reveals hypoechoic islands surrounded by hyperechoic bundles in the deep dermis and in the subcutaneous cellular tissue. The literature contains few references to ultrasound assessment of CFH. Cambiaghi et al.5 present a series of 3 cases and report on the usefulness of ultrasound in the differential diagnosis, although they do not describe or present their imaging findings. Grilo et al.6 describe CFH as a poorly defined, homogeneous, slightly hyperechoic lesion adjacent to the subcutaneous cellular tissue; however, their report does not show the ultrasound image. Our search of the literature revealed only 4 ultrasound images, and, despite differences in the descriptions, each of the 4 images shows findings similar to those we report.2,7–9 It seems reasonable to think that the more or less hypoechoic appearance of the lesion depends on the amount of adipose tissue in the hamartoma.
Fibrolipomatous hamartoma affecting a nerve is located at a deeper level and is observed as hypoechoic thickening of the nerve on ultrasound,10 since both fibrous and adipose tissue present higher echogenicity than the nerve.
Given that CFH is not accompanied by increased blood flow, color Doppler can facilitate the differential diagnosis with vascular lesions such as infantile hemangioma, congenital hemangioma, or specific vascular malformations. Other lesions that can be confused with CFH can be ruled out using ultrasound (Table 1).
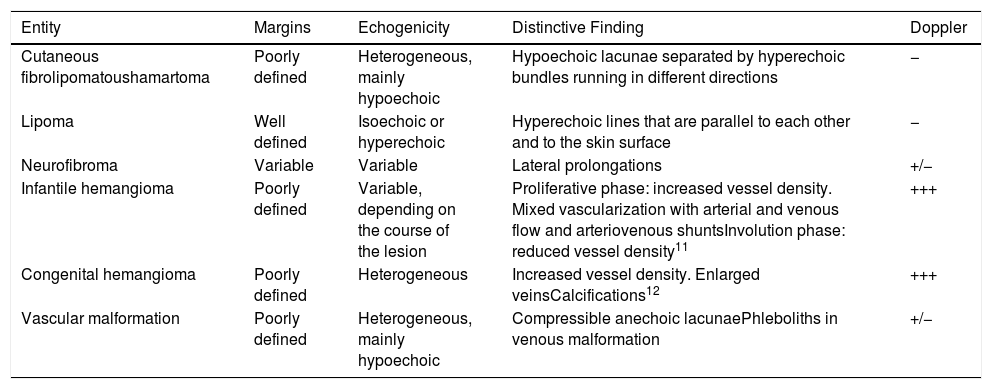
Ultrasound of Cutaneous Fibrolipomatous Hamartoma and of Entities Included in the Differential Diagnosis.
| Entity | Margins | Echogenicity | Distinctive Finding | Doppler |
|---|---|---|---|---|
| Cutaneous fibrolipomatoushamartoma | Poorly defined | Heterogeneous, mainly hypoechoic | Hypoechoic lacunae separated by hyperechoic bundles running in different directions | − |
| Lipoma | Well defined | Isoechoic or hyperechoic | Hyperechoic lines that are parallel to each other and to the skin surface | − |
| Neurofibroma | Variable | Variable | Lateral prolongations | +/− |
| Infantile hemangioma | Poorly defined | Variable, depending on the course of the lesion | Proliferative phase: increased vessel density. Mixed vascularization with arterial and venous flow and arteriovenous shuntsInvolution phase: reduced vessel density11 | +++ |
| Congenital hemangioma | Poorly defined | Heterogeneous | Increased vessel density. Enlarged veinsCalcifications12 | +++ |
| Vascular malformation | Poorly defined | Heterogeneous, mainly hypoechoic | Compressible anechoic lacunaePhleboliths in venous malformation | +/− |
This case of unilateral precalcaneal CFH illustrates the usefulness of ultrasound in the differential diagnosis of this lesion. Therefore, we believe that high-frequency ultrasound is a useful technique for confirming a clinical suspicion of CFH and can obviate the need for biopsy at a site that is particularly painful and where scarring can cause chronic discomfort. Furthermore, ultrasound enables us to reassure parents by showing and explaining the lesion to them.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Rodríguez-Bandera AI, Feito-Rodríguez M, de Lucas-Laguna R. Imagen clínica y ecográfica de un hamartoma fibrolipomatoso cutáneo. Actas Dermosifiliogr. 2019;110:513–515.


