





Per-visit fees and the characteristics of private practice in dermatology have been studied very little, at least in Spain. This study aims to describe how dermatologists in private practice in Spain provide services, collect payment, promote their services, and establish fees. We also analyze differences by region, age, and sex.
Materials and methodsWe performed a descriptive, cross-sectional study based on an online questionnaire with a total of 31 questions aimed exclusively at dermatologists in private practice in Spain. The questionnaire was open for responses from May 17 to June 5, 2018. The data were analyzed by comparing region, sex, and age.
ResultsA total of 234 questionnaires were returned, with equal numbers of male and female respondents and proportional numbers in terms of the regional sections of the Spanish Academy of Dermatology and Venereology (AEDV). Some differences were found for region, age, and sex. The fees of female dermatologists were consistently lower, even after adjusting for confounding factors by means of regression models.
ConclusionsWe have described the characteristics of private dermatology practice in Spain. Charging of lower fees by female dermatologists requires more detailed study, probably using qualitative research techniques.
Las tarifas por acto médico y los hábitos de asistencia privada de los dermatólogos apenas han sido objeto de estudio, al menos en nuestro entorno inmediato. Con el presente trabajo pretendemos describir hábitos de prestación de servicios, medios de cobro, promoción y fijación de tarifas de los dermatólogos que realizan asistencia privada en España. Secundariamente, buscamos analizar las diferencias por sección territorial, edad y sexo.
Materiales y métodosEstudio descriptivo transversal a partir de un cuestionario on-line con un total de 31 preguntas dirigido exclusivamente a dermatólogos con asistencia privada en España, abierto a respuestas del 17 de mayo al 5 de junio de 2018. Los datos fueron analizados comparando por sección territorial, sexo y edad.
ResultadosSe recibió un total de 234 respuestas, paritarias en cuanto a sexo y proporcionadas en cuanto a las secciones territoriales de la Academia Española de Dermatología y Venereología (AEDV). Pudieron constatarse algunas diferencias por sección territorial, edad y sexo. Destacaban las tarifas sistemáticamente menores de las dermatólogas, incluso tras ajustar por factores de confusión mediante modelos de regresión.
ConclusionesQuedan descritas características de la asistencia privada en Dermatología en España. El hecho de que haya tarifas más baratas entre las dermatólogas requiere de un estudio más detallado, probablemente mediante técnicas de investigación cualitativa.
Remuneration of specialist doctors is the subject of analysis and debate, not only in terms of salary,1–4 but also with regard to how services are billed. While some studies have analyzed payment models in non-English-speaking Europe (the first of these were performed in the middle of the 20th century5), most studies that deal with payment of doctors per patient or per intervention come from the English-speaking world.6–12 Recently, some authors have criticized regional differences in financial compensation because of the inequality this may generate in the geographic distribution of dermatologists.13
Private health are in Spain is growing.14 Part of this growth is a result of cutbacks in public spending (and the subsequent transformation of the health care system), diversification of supply, and changes in patterns of demand.15 Another factor that explains this growth in our specialty is the growing trend of esthetic procedures.16
After reviewing the literature, we found no scientific publications to date that show the variations in fees per intervention and payment-collection habits among dermatologists providing private care in the different autonomous communities in Spain. Spanish studies examine general aspects of private care14 or pay conditions of doctors in all specialties.1
We consider the description of the characteristics and fees of specialists in medical and surgical dermatology and venereology who provide private care in Spain in 2018 to be important from a scientific, sociological, and historical perspective. This snapshot of the current economic situation in dermatology makes it possible to determine the current state of private care in this specialty, how it is developing, and which areas require criticism or improvement; it is also an historical testament to the social and economic environment.
The primary goal of this study was to describe the characteristics of private dermatology practice and the fees for the most common medical and esthetic procedures. The secondary goal was to analyze these fees by region, age, and sex.
Material and MethodsWe carried out an online survey (Appendix B; questions are shown in Supplementary Table 1), which was open for responses from 17 May to 5 June, 2018.
Demographic Data and Professional Affiliation.
| Variable | Results |
|---|---|
| Sex | Male: 117 (50%) |
| Female: 117 (50%) | |
| Age | Under 40 years of age: 64 (27.4%) |
| 40-50 years of age: 56 (23.9%) | |
| 50-60 years of age: 79 (33.8%) | |
| Over 60 years of age: 35 (15.0%) | |
| Regional section to which you belong | Andalusia: 45 (19.2%) |
| Asturias–Cantabria–Castillia-Leon: 12 (5.1%) | |
| Balearic Islands: 5 (2.1%) | |
| Canary Islands: 6 (2.6%) | |
| Catalonia: 14 (6.0%) | |
| Center: 67 (28.6%) | |
| Galicia: 35 (15.0%) | |
| Murcia: 7 (3.0%) | |
| Valencia: 19 (8.1%) | |
| Basque Country-Navarre-Aragon-Rioja: 24 (10.3%) | |
| Usual practice activity | Private only: 95 (40.6%) |
| Mostly private with some public: 45 (19.2%) | |
| Mostly public with some private: 94 (40.2%) | |
| Type of private clinic | Own/dermatologist-owned clinic with up to 4 doctors on the team: 118 (50.4%) |
| Own/dermatologist-owned clinic with >4 doctors: 21 (9.0%) | |
| Medical center/polyclinic with several specializations: 51 (21.8%) | |
| Large hospital/private clinic: 44 (18.8%) |
Requests for responses were sent through the following professional forums with access controlled by dermatologists: Foroderma 2.0 (Facebook group with 668 members at the date of closure of the survey), Dermachat (chat forum with 340 members on the closure date), and Dermus (dermatologists who attended the 11th Meeting of Private Dermatology and New Technologies [XI Reunión de Dermatología Privada y Nuevas Tecnologías], held in Madrid from May 31 to June 2, 2018). This meant that all respondents were medical specialists in medical and surgical dermatology and venereology. Although these groups consist of mostly Spanish members, the introduction to the survey and the initial questions excluded any specialist not working in Spain. Responses were only accepted from professionals carrying out private practice (ensured by an exclusion question at the start of the survey).
Data were analyzed using the χ2 test, comparing region, sex, and age. Questions regarding fees were asked in terms of categories to make the survey more acceptable. In order to analyze these data, each category was recoded as its mean value (assuming that fees are distributed uniformly in each category) and the mean fees of the extreme categories were estimated (Appendix B, Supplementary Table 2). The fees were compared using analysis of variance (ANOVA) and linear regression after verifying that these techniques were applicable. To evaluate the factors that affect fees by sex, we performed successive linear regression models, including the variables sex, age, autonomous community, type of center, and a variable for interaction between sex and age. The SPSS (version 20.0) and Stata (version 15) statistical software packages were used for the statistical analysis. Results of the tests were assumed to be significant for values of p<.05.
Payment-Collection, Promotion and Price-Change Habits.
| Variable | Results |
|---|---|
| Person/s who collect payment for medical interventions in the center | The specialist who performed the intervention: 8 (3.4%) |
| Auxiliary, clinical, hired nursing personnel: 35 (15.0%) | |
| Secretary, receptionist: 138 (59.0%) | |
| Personnel of the clinic or medical center: 53 (22.6%) | |
| Payment-collection in advance of interventions | Never: 213 (91.0%) |
| Occasionally, in specific interventions that require expenditure of material or prior preparation (e.g. injectable polylactic acid): 15 (6.4%) | |
| Often: 6 (2.6%) | |
| Acceptance of payment in cash | Yes: 225 (96.2%) |
| No: 9 (3.8%) | |
| Acceptance of payment by bank card | Yes: 60 (25.6%) |
| No: 174 (74.4%) | |
| Acceptance of payment via online banking | Yes: 60 (25.6%) |
| No: 174 (74.4%) | |
| Acceptance of payment via virtual currency or blockchain | No: 214 (91.5%) |
| Yes: 19 (8.1%) | |
| No, but I am considering it in the near future: 1 (0.4%) | |
| Acceptance of payment by barter (exchange of services) | Never: 211 (90.2%) |
| Rarely: 23 (9.8%) | |
| Usually: 0 (0%) | |
| Do you provide treatment vouchers (session packs) for esthetic treatment? | Yes: 28 (12.0%) |
| Yes, but only for a few treatments/techniques: 50 (21.4%) | |
| Never: 107 (45.7%) | |
| Prefers not to answer/not applicable: 49 (20.9) | |
| Do you provide financing options for treatments? | No, and I am not considering it: 133 (56.8%) |
| No, but I am considering it: 15 (6.4%) | |
| Rarely: 23 (9.8%) | |
| Usually: 11 (4.7%) | |
| Prefers not to answer/not applicable: 52 (22.2%) | |
| Do you provide a discount for consultations by several family members in the same visit? | Never: 43 (18.4%) |
| Rarely: 101 (43.2%) | |
| Always: 83 (35.5%) | |
| Prefers not to answer/not applicable: 7 (3.0%) | |
| How often do you change/revise your fees? | Each year, in line with the consumer price index: 15 (6.4%) |
| Every 2 years: 33 (14.1%) | |
| Every 3-5 years: 45 (19.2%) | |
| In periods of more than 5 years: 46 (19.7%) | |
| Only when I consider it appropriate: 95 (40.6%) |
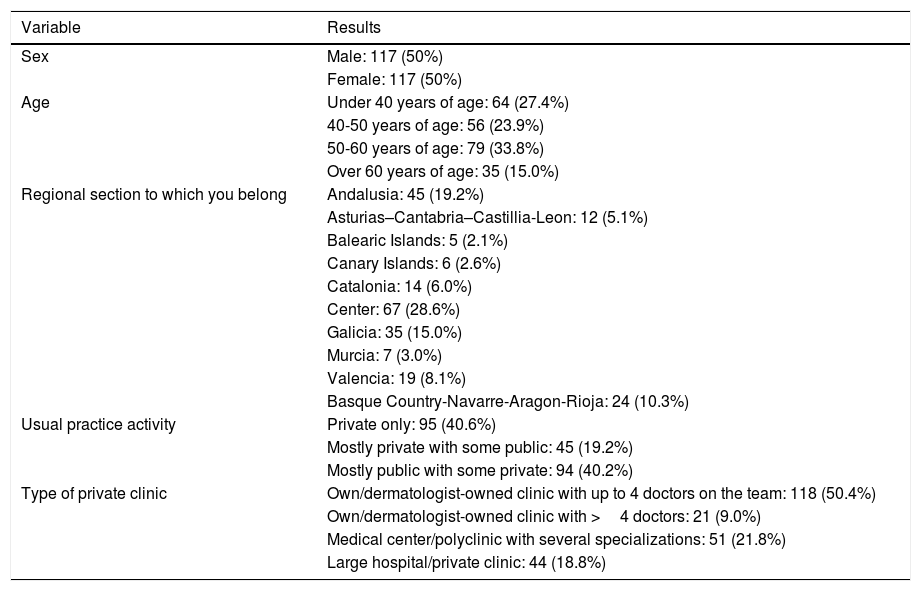
A total of 234 specialists in medical and surgical dermatology and venereology who carry out private care in Spain (117 men [50%] and 117 women [50%]) responded to the survey. The demographic and professional-affiliation data of the survey respondents are shown in Table 1.
All age groups were represented (Fig. 1). Although fewer women over the age of 60 years responded (11% compared to 19%), the difference was not significant.

Responses were received from all the regional sections of the Spanish Academy of Dermatology and Venereology (AEDV) and the distribution in the sample was similar to that of AEDV dermatologists (compared with the updated numbers by section available from the AEDV; p=.23). Statistically significant differences were found with respect to the age of the dermatologists who responded to the survey in the different sections (p=.007): more responses were received from the youngest age group in the Center (34.4% of all those under 40 years of age), Andalusia (21.9%), and Galicia (14.1%) sections, and from the oldest age group in the Center (25.7% of all those over 60 years of age), Valencia (22.9%), and Galicia (17.1%) sections.
The activity or type of professional practice of the surveyed dermatologists (with three response options: exclusively private practice, mostly public practice with some private practice, or mostly private practice with some public practice) presented statistically significant differences in terms of age (p=.01), with predominantly private care among the older age groups (Fig. 2).

Most of the surveyed dermatologists (50.4%) work in their own clinics or in clinics of up to 4 doctors. In the sample, the most common types of private clinic are distributed unequally between the sections (p=.008) (dermatologist's own clinic with a small team, dermatologist's own clinic with a large team/polyclinics, and large hospitals/clinics). Thus, for example responses were received from dermatologists with their own clinics and a large team only in the Center, Catalonia, Valencia and Galicia sections. Figure 3 shows the different types of practice by age (p=.003).

Habits and Methods of Payment Collection, Promotion and Price Changes
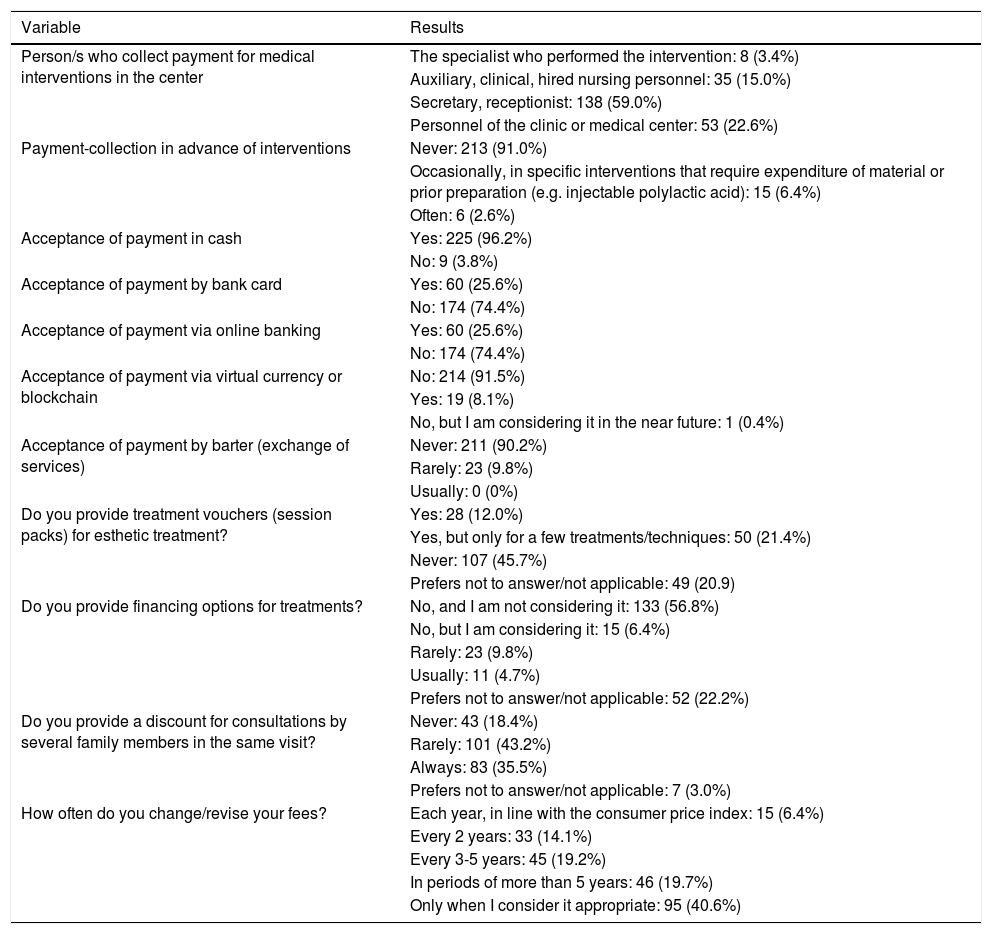
The results regarding habits and methods of payment collection, promotions and price changes, and the presence or absence of significant differences in terms of regional section, sex, and age, are summarized in Table 2.
In terms of who collects payment, the most common response is that dermatologists delegate this responsibility to their secretaries, receptionists or personnel of the medical center itself (81.6%). Fifteen percent of those surveyed delegate this task to nursing staff. Only 9% of dermatologists collect payment before performing some techniques (this is more frequently an exceptional practice).
Most specialists accept payment in cash (96.2%) and bank card (75.2%). The percentage of specialists who accept bank cards differed by regional section (p=.008): 100% in the Canary Islands section and lower percentages in the Galicia (54.3%) and Murcia (42.9%) sections. The percentage also differed according to age (p=.037); accepting payment by bank card was more common among younger dermatologists (85.9% of those below 40 years of age accept card payment) and less common among older dermatologists (62.9% of those over 60 years of age accept card payment).
Other means of paying fees, such as online banking, also show a high percentage of acceptance (67.1%). Other more novel systems, however, such as payment via cryptocurrency, are still poorly accepted: only one dermatologist accepted this form of payment, although 8.1% of all respondents were considering including it. Payment by barter is rare, though more common among men (13.7% stated that they occasionally accepted barter) than among women (6%), with statistically significant differences (p=.048).
Three pieces of data stood out in terms of financing and promotions. First, most specialists (81.3%) do not provide financing for treatments (6.4% were considering providing it). Second, fewer than half of dermatologists provide vouchers for techniques or treatments (42.1%) and this practice is more commonly used for just a few treatments (64.1% of those provided) and by younger dermatologists (Fig. 4; p=.01). Third, it is common for discounts to be applied occasionally to family groups (81.1%).

Finally, the rate at which fees are changed showed significant differences by both sex and age. Male dermatologists tend to revise their consultation fees over shorter and more defined periods of time (65% have an established time period for adjusting fees), whereas female dermatologists more frequently change their fees when they deem it appropriate or over longer periods (66.7% do so in periods of more than 5 years or only when they deem it appropriate) (p=.009). Dermatologists over 50 years of age more frequently have a defined period for changing prices (p=.001) (Fig. 5).
Habits in Terms of Price-Setting and Provision of Services
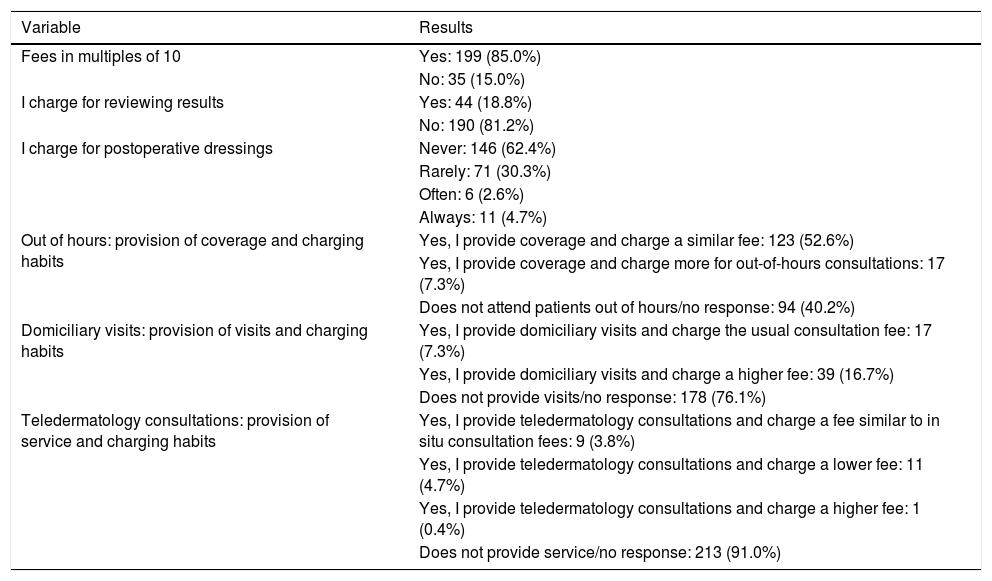
The summary of the results regarding habits in terms of establishing fees and the presence or absence of significant differences in terms of regional section, sex, and age, are shown in Table 3.
Habits in Price-Setting and Provision of Services.
| Variable | Results |
|---|---|
| Fees in multiples of 10 | Yes: 199 (85.0%) |
| No: 35 (15.0%) | |
| I charge for reviewing results | Yes: 44 (18.8%) |
| No: 190 (81.2%) | |
| I charge for postoperative dressings | Never: 146 (62.4%) |
| Rarely: 71 (30.3%) | |
| Often: 6 (2.6%) | |
| Always: 11 (4.7%) | |
| Out of hours: provision of coverage and charging habits | Yes, I provide coverage and charge a similar fee: 123 (52.6%) |
| Yes, I provide coverage and charge more for out-of-hours consultations: 17 (7.3%) | |
| Does not attend patients out of hours/no response: 94 (40.2%) | |
| Domiciliary visits: provision of visits and charging habits | Yes, I provide domiciliary visits and charge the usual consultation fee: 17 (7.3%) |
| Yes, I provide domiciliary visits and charge a higher fee: 39 (16.7%) | |
| Does not provide visits/no response: 178 (76.1%) | |
| Teledermatology consultations: provision of service and charging habits | Yes, I provide teledermatology consultations and charge a fee similar to in situ consultation fees: 9 (3.8%) |
| Yes, I provide teledermatology consultations and charge a lower fee: 11 (4.7%) | |
| Yes, I provide teledermatology consultations and charge a higher fee: 1 (0.4%) | |
| Does not provide service/no response: 213 (91.0%) |
Eighty-five percent of respondents establish their fees in multiples of 10. The majority of respondents do not charge for reviewing test results (81.2%); the same is true for postoperative dressings, which are either not charged for or charged for only rarely (92.7%). Out-of-hours consultations are performed by 59.9% of dermatologists, of whom 17 (8.3 of all respondents) charge a higher fee for these consultations, with significant differences by age (p=.002). A total of 31.6% of male dermatologists and 16.2% of female dermatologists (p=.001) carry out domiciliary visits, for which they frequently charge a higher fee than for visits at the clinic (16.7% vs 7.3%). These visits are more frequently carried out by older dermatologists: 37.1% of those over 60 years of age stated that they carried out domiciliary visits compared to 11.5% of those under 40 years of age (p=.037). Only 9% of the dermatologists surveyed provide teledermatology consultations – mostly for the same price or lower than for an in situ visit.
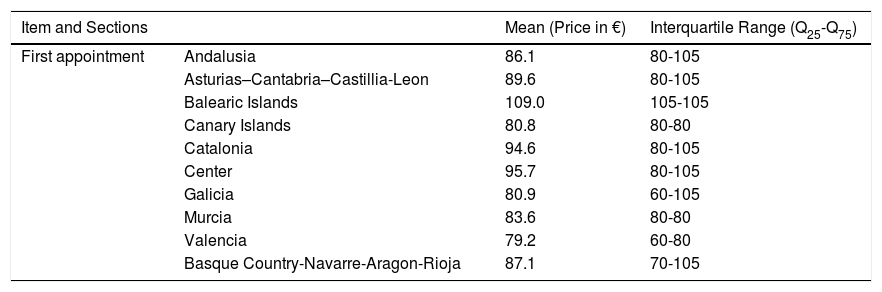
FeesThe fees for the different items surveyed are shown in Table 4. Below, we discuss differences in price by regional section and age.
Fees Established by the Surveyed Dermatologists.
| Item and Sections | Mean (Price in €) | Interquartile Range (Q25-Q75) | |
|---|---|---|---|
| First appointment | Andalusia | 86.1 | 80-105 |
| Asturias–Cantabria–Castillia-Leon | 89.6 | 80-105 | |
| Balearic Islands | 109.0 | 105-105 | |
| Canary Islands | 80.8 | 80-80 | |
| Catalonia | 94.6 | 80-105 | |
| Center | 95.7 | 80-105 | |
| Galicia | 80.9 | 60-105 | |
| Murcia | 83.6 | 80-80 | |
| Valencia | 79.2 | 60-80 | |
| Basque Country-Navarre-Aragon-Rioja | 87.1 | 70-105 | |
| Item in Overall Regional Sections | Mean (Price in €) | Interquartile Range (Q25-Q75) |
|---|---|---|
| First Appointment | 80 | 80-105 |
| Check-up | 60 | 40-80 |
| Low-complexity surgery (e.g. shaving a nevus) | 150 | 75-150 |
| Medium-complexity surgery (e.g. removal of a tumor on the torso or a small or medium tumor on the face with direct closure) | 150 | 150-250 |
| High-complexity surgery (e.g. removal of a large tumor on the torso or a large tumor on the face with complex closure by means of flap or graft) | 250 | 150-350 |
| Infiltration of botulinum toxin in a small anatomic area (e.g. between the eyebrows), including material | 250 | 150-400 |
| Infiltration of a vial of hyaluronic acid, including material | 350 | 250-350 |
The mean fee for a first appointment as a private patient in Spain at the time of the survey was €88.60. This was the only one of the fees surveyed that showed statistically significant differences between regional sections (p=.044) (Table 4).
The only one of the fees investigated that showed statistically significant differences by age was the fee for surgery of medium complexity (p=.019).
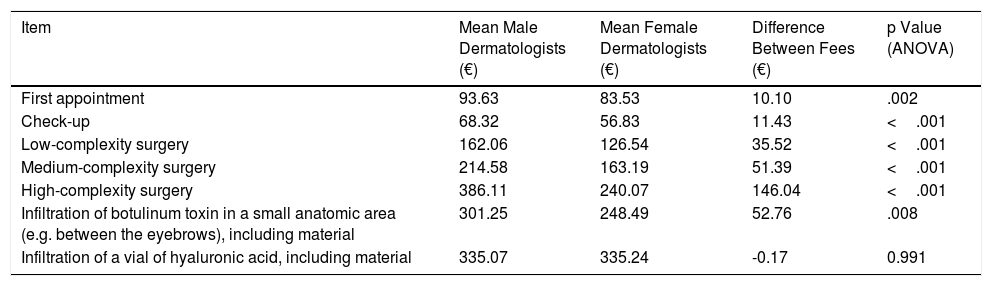
Differences in fees by sex of the dermatologists surveyed are a different matter. The survey found that female dermatologists charge lower fees than male dermatologists for all items surveyed except one. Fees for first appointments, check-ups, low-complexity surgery, medium-complexity surgery, high-complexity surgery, and administration of botulinum toxin in a small area were all charged at a lower price by female dermatologists; the only item with no significant differences was administration of hyaluronic acid (Table 5). Application of successive multiple linear regression models, adding the variables age, community, type of center, and a variable for interaction between age and sex showed no major changes in differences between fees, thus ruling out these factors as an explanation of the differences.
Differences in Fees Based on Sex of Specialist.
| Item | Mean Male Dermatologists (€) | Mean Female Dermatologists (€) | Difference Between Fees (€) | p Value (ANOVA) |
|---|---|---|---|---|
| First appointment | 93.63 | 83.53 | 10.10 | .002 |
| Check-up | 68.32 | 56.83 | 11.43 | <.001 |
| Low-complexity surgery | 162.06 | 126.54 | 35.52 | <.001 |
| Medium-complexity surgery | 214.58 | 163.19 | 51.39 | <.001 |
| High-complexity surgery | 386.11 | 240.07 | 146.04 | <.001 |
| Infiltration of botulinum toxin in a small anatomic area (e.g. between the eyebrows), including material | 301.25 | 248.49 | 52.76 | .008 |
| Infiltration of a vial of hyaluronic acid, including material | 335.07 | 335.24 | -0.17 | 0.991 |
The figures in bold type indicate significant differences and the size of the corresponding p value.
In this study, we describe the characteristics and fees in private care provided by specialists in dermatology working in Spain. Some differences were found based on the sex, age, and geographic location of the dermatologists, notably including greater presence of older dermatologists in private practice, different acceptance rates for credit cards by regional section, and differences in fee changes by age and sex. In terms of fees, differences were observed in the price of first appointments by regional section, and in practically all fee items by sex, where the fees set by female dermatologists were significantly lower than those set by male dermatologists.
We have been unable to identify similar publications in the literature. Unlike the analyses of the consequences of certain types of payment in the English-speaking world,6–12 Spanish studies focus on general aspects of private care14 or pay conditions of doctors in all specialties.1 The survey sample included equal numbers of male and female respondents and was proportional with respect to the number of academic belonging to each regional section of the AEDV. Furthermore, measures were taken to prevent social desirability bias (consisting of giving answers in the survey that are closer to what is socially more acceptable)17; this was achieved essentially by means of anonymous data collection and processing) and to facilitate participation (such as category-based questions). The study may, however, have some limitations, such as the relatively small sample size (although it represents more than 10% of academics and, therefore, of dermatologists in Spain18), its selection, and the restrictions on representativeness that may result from the differences in age, geographic area, and type of private clinic.
The ages shown in the survey correspond to the current demographics of health care professionals.1 It can be stated that the older Spanish dermatologists are, the more frequently they work in private practice. While there are approximately 3000 private medical centers in Spain and the majority of the turnover (€3,96 million in 2015) comes from 9 main actors (large hospital groups and insurers),14 dermatologists usually work in small clinics (their own clinics, with up to 4 doctors on the team). Clinics owned by dermatologists and with more than 4 doctors on the team are the exception and are restricted to a few geographic areas.
At present, teledermatology consultations are rare. Domiciliary visits by dermatologists are rare and, in general, more common among male dermatologists. In terms of payment-collection habits, we can conclude that most dermatologists tend to delegate this responsibility to administrative personnel, payment is rarely collected in advance, and financing of treatments or the provision of vouchers is also rare. Notable discrepancies were observed in terms of acceptance of payment by bank card, with 100% acceptance in the Canary Islands (possibly owing to the tax-deductible nature of medical expenses included in the Canary Islands 2018 budget with effects retroactive to 2017, which requires submission of proof of payment by bank card, transfer or check19) and lower rates of acceptance in other sections (probably linked to tax-related differences between autonomous communities). It is also of note that most dermatologists set their fees in multiples of 10 and do not adjust them in accordance with the consumer price index. The fact that fees are rounded is probably due to convenience when collecting payment in cash and providing change; a similar reason may explain why prices are updated in increments of 10. The fact that older dermatologists usually have a more established system of setting fees may indicate that experience provides them with greater financial education.
With regard to fees, the differences in the price of a first appointment are linked to the presence of extreme values in certain geographic areas. Nevertheless, the values are relatively uniform between regional sections. While no differences were observed in nearly any of the fees by age of the dermatologist, medium-complexity surgery (performed privately by most of the specialists surveyed) show a tendency to be charged at a higher rate by older dermatologists. Highly complex surgery is performed by a smaller proportion of dermatologists and by an even smaller proportion of older dermatologists.
The most surprising finding in our survey is that female dermatologists charge lower fees than male dermatologists. We do not know the reasons for this. These findings are in line with a recent publication that observed mean differences of €12,000 in annual salaries (to the detriment of female doctors) in Spain,1 but in our study, it is noteworthy that the differences are not in overall salary but in fee per medical intervention and probably self-imposed.
ConclusionsWe believe that this study may serve as a frame of reference for understanding the habits of Spanish dermatologists providing private care. The fact that the fees of female dermatologists are lower requires more detailed study —probably using qualitative research techniques.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
The authors would like to thank all those who responded to the survey and especially the members of the Dermchat and Foroderma 2.0 communities, for their generosity in responding to the survey and for being a source of inspiration and encouragement in overcoming the daily vicissitudes of dermatology.
Please cite this article as: Martin-Gorgojo A, García-Doval I, del Río de la Torre E. Survey on Private Dermatology Practice Characteristics and Fees in Spain in 2018. Actas Dermosifiliogr. 2019;110:137–145.


