
Treatment of advanced cutaneous squamous cell carcinoma (CSCC) is complex, and no specific drugs have been approved. CSCC carries a high mutational burden and is associated with immunosuppression,1 suggesting that it is a potential target for immunotherapy.
The United States Food and Drug Administration (FDA) recently approved cemiplimab, an anti–programmed cell death 1 antibody, for the treatment of metastatic or locally advanced CSCC that cannot be treated with curative radiotherapy or surgery.2 Approval was based on the results of 2 trials: R2810-ONC-1423 (Trial 1), a phase 1 multicenter, open-label, dose-finding clinical trial in patients with a variety of advanced solid tumors3; and R2810-ONC-1540 (Trial 2), a multicenter phase 2 open-label, nonrandomized, 3-arm clinical trial (2 arms with metastatic CSCC and cemiplimab every 2 or 3 weeks and 1 arm with locally advanced CSCC and cemiplimab every 2 weeks).4
Trial 1 included 26 patients and Trial 2 included 82 patients. Of these 108 patients, 33 had locally advanced CSCC and 75 metastatic CSCC (69% distal and 31% nodal). Mean age was 71 years, 85% of patients were men, 97% were white, 50% had received ≥ 1 systemic cancer therapy, 96% had undergone surgery, and 79% had undergone radiotherapy. No immunocompromised patients were included. All patients received intravenous cemiplimab 3 mg/kg every 2-3 weeks until disease progression, unacceptable toxicity, or a maximum of 48 weeks (Trial 1) or 96 weeks (Trial 2). Tumor response was evaluated every 8 weeks. The main efficacy objectives were the objective response rate (ORR) and duration of response. These objectives were evaluated by an independent review board in line with the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1, based on radiological data and digital photography. The intention-to-treat analysis revealed an ORR of 47% (95% CI, 38%-57%) (4% complete response and 44% partial response). The ORR was similar in metastatic CSCC and in locally advanced CSCC (47% and 49%, respectively). The median duration of response had not been reached at the time of the analysis (range, 1.0-15.2 months; ≥ 6 months in 61%). The median time to response was approximately 2 months.2
Migden et al.5 recently published these results in part. The authors included all the patients from Trial 1 (n = 26), although only those with metastatic CSCC and cemiplimab every 2 weeks from Trial 2 (n = 59). The ORR in the intention-to-treat analysis was 50% and 47%, respectively. As for the safety profile, more than 50% experienced adverse effects (AEs). The most frequent were fatigue, rash, and diarrhea. Treatment had to be suspended owing to AEs in 7% of patients. The most common grade 3-4 AEs were cellulitis, sepsis, arterial hypertension, and pneumonia. Immunological AEs were noteworthy (Table 1). Eleven patients died during the trials; 3 of the deaths were attributed to treatment with cemiplimab.
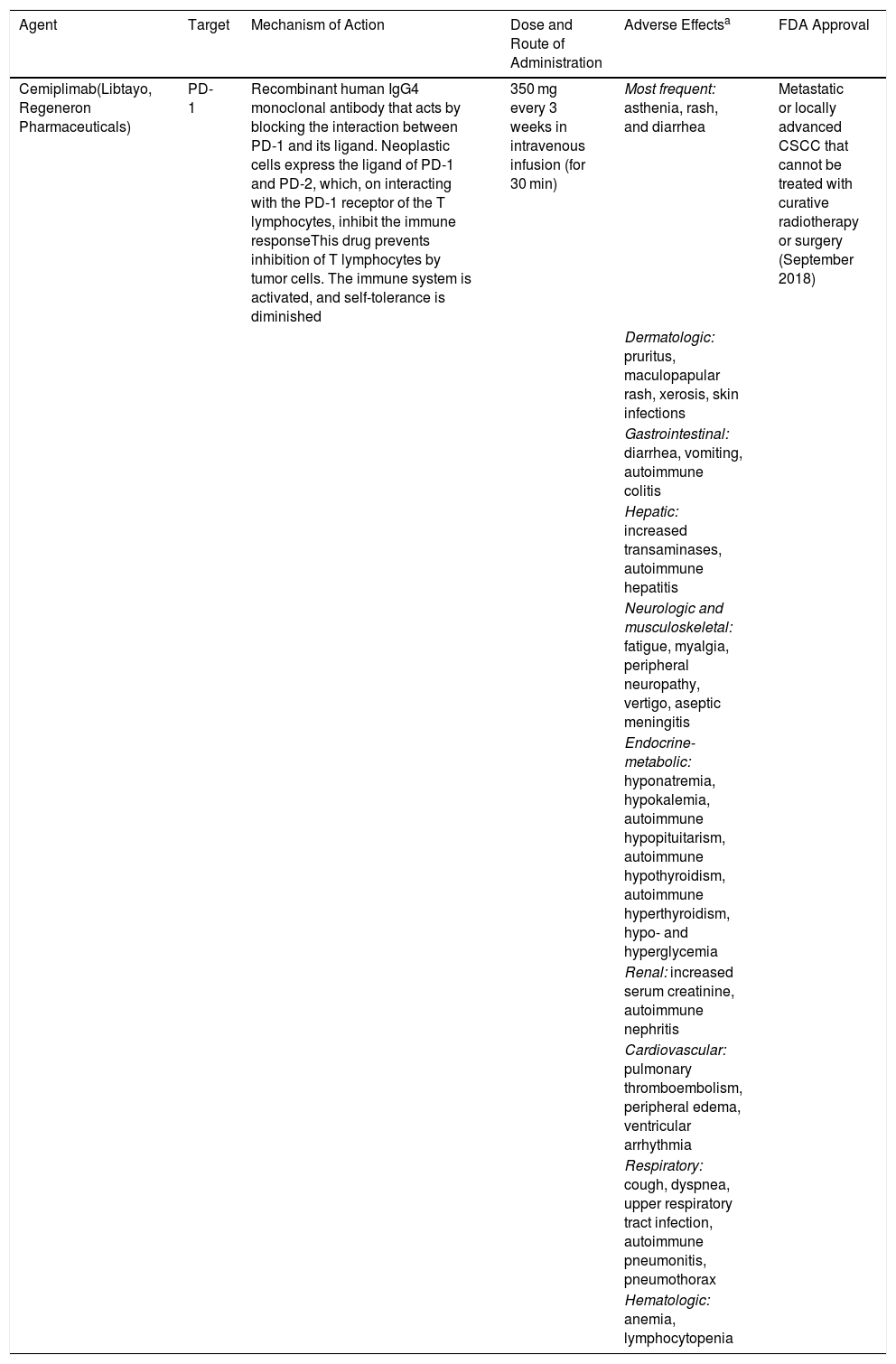
New Immunotherapeutic Agents Used in Advanced Cutaneous Cancer.
| Agent | Target | Mechanism of Action | Dose and Route of Administration | Adverse Effectsa | FDA Approval |
|---|---|---|---|---|---|
| Cemiplimab(Libtayo, Regeneron Pharmaceuticals) | PD-1 | Recombinant human IgG4 monoclonal antibody that acts by blocking the interaction between PD-1 and its ligand. Neoplastic cells express the ligand of PD-1 and PD-2, which, on interacting with the PD-1 receptor of the T lymphocytes, inhibit the immune responseThis drug prevents inhibition of T lymphocytes by tumor cells. The immune system is activated, and self-tolerance is diminished | 350 mg every 3 weeks in intravenous infusion (for 30 min) | Most frequent: asthenia, rash, and diarrhea | Metastatic or locally advanced CSCC that cannot be treated with curative radiotherapy or surgery (September 2018) |
| Dermatologic: pruritus, maculopapular rash, xerosis, skin infections | |||||
| Gastrointestinal: diarrhea, vomiting, autoimmune colitis | |||||
| Hepatic: increased transaminases, autoimmune hepatitis | |||||
| Neurologic and musculoskeletal: fatigue, myalgia, peripheral neuropathy, vertigo, aseptic meningitis | |||||
| Endocrine-metabolic: hyponatremia, hypokalemia, autoimmune hypopituitarism, autoimmune hypothyroidism, autoimmune hyperthyroidism, hypo- and hyperglycemia | |||||
| Renal: increased serum creatinine, autoimmune nephritis | |||||
| Cardiovascular: pulmonary thromboembolism, peripheral edema, ventricular arrhythmia | |||||
| Respiratory: cough, dyspnea, upper respiratory tract infection, autoimmune pneumonitis, pneumothorax | |||||
| Hematologic: anemia, lymphocytopenia |
Source: Migden et al.5
Abbreviations: CSCC, cutaneous squamous cell carcinoma; PD-1, programmed cell death protein 1.
Immunotherapy is revolutionizing the treatment of advanced cutaneous cancer. Cemiplimab is the first drug to be approved for the treatment of advanced CSCC. The many issues that have yet to be resolved include its role in adjuvant and neoadjuvant treatment, its efficacy in immunocompromised patients, long-term safety (including mortality attributed to the drug), and the high cost of therapy. It is essential that dermatologists become familiar with these new agents and their AEs.
Please cite this article as: Morgado-Carrasco D, et al. FR-Cemiplimab, primer fármaco aprobado para el tratamiento del carcinoma cutáneo de células escamosas metastásico o irresecable. Actas Dermosifiliogr. 2020;111:161–163.


