


A 56-year-old man attended our unit because he had noticed an increase in the size of his right nipple over the previous 4 years. His past medical and drug history were unremarkable.
He denied both trauma and application of topical products to the area. While he reported a general absence of pain in the region, he did mention that he sometimes experienced local irritation he attributed to friction from clothing.
The findings of an ultrasound performed at another hospital were unremarkable, and showed skin with smooth, regular outlines and normal thickness of the subcutaneous tissue.
The physical examination showed a slightly erythematous papule on the right nipple (Fig. 1) that was hard to the touch but not painful when palpated. The intramammary and axillary lymph nodes were not enlarged.
Histopathology
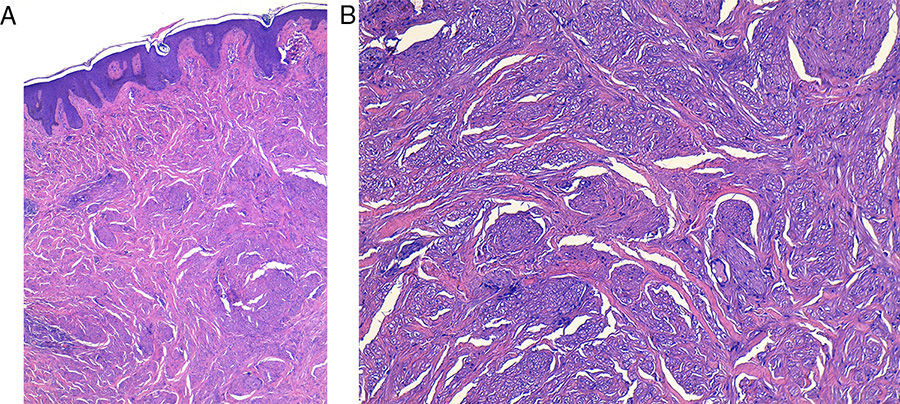
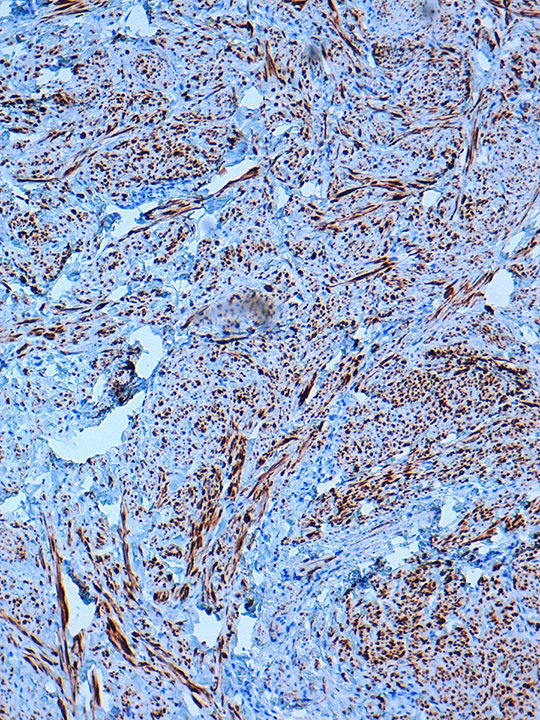
Hematoxylin-eosin staining showed a noncapsulated poorly circumscribed proliferation of interlaced spindle cells with an irregular eosinophilic cytoplasm in the dermis (Fig. 2 A,B). There was no mitosis or cellular atypia. In the immunohistochemical study, the cells stained positive for desmin (Fig. 3).


What Is Your Diagnosis?
DiagnosisLeiomyoma of the nipple.
Clinical Course and TreatmentGiven the benign nature of the condition and the fact that the lesion was asymptomatic, it was decided to take a watch-and-wait approach.
CommentLeiomyomas are rare benign smooth muscle tumors that typically develop in the genitourinary or gastrointestinal tract, and less frequently in the skin.1 Cutaneous leiomyomas are classified as piloleiomyomas (derived from the arrector pili muscle), angioleiomyomas (derived from vascular wall smooth muscle), and genital leiomyomas (derived from scrotal, vulvar, or nipple smooth muscle).
Based on reports in the literature, leiomyoma of the nipple appears to be more common in women,2 and tends to present as a long-standing papule that is asymptomatic or causes occasional episodes of sharp pain. This pain is thought to be due to the contraction of neoplastic smooth muscle fibers in the tumor bed and is induced by friction or can appear spontaneously.1,4
The nipples are typically asymmetric in the physical examination and the tumor is the same color as the surrounding skin and firm to the touch The differential diagnosis should include Paget disease, leiomyosarcoma, adenoma, fibroma, and papilloma of the nipple.2–4 These entities must be ruled out histologically.
The most remarkable histologic finding is the presence of a noncapsulated, irregular mass in the dermis comprising an anomalous proliferation of smooth muscle spindle cells with an eosinophilic cytoplasm that stain positive with the muscle differentiation markers actin and desmin in the immunohistochemical study. These cells are arranged as interlacing bundles within a stroma of connective tissue. The absence of cellular atypia and mitosis is an important finding for differentiating leiomyoma from leiomyosarcoma.2,3
Recent reports have described the identification of estrogen and progesterone receptors in nipple leiomyoma biopsy specimens and the development of leiomyoma in patients receiving hormonal drugs, such as tamoxifen, although more studies are necessary to confirm these observations.1,4–6 Although we did not study the association between leiomyoma and hormones in our patient, the above findings suggest that the association between genital leiomyoma and sex hormones is indeed a possibility.
Treatment of leiomyoma of the nipple varies according to symptoms. Calcium-channel and alpha-adrenergic blockers have proven effective in controlling pain induced by smooth muscle contraction, and surgery and even carbon dioxide laser therapy are also an option for symptomatic lesions.2–4
Please cite this article as: Brugués A, Alós L, Fuertes de Vega I. Nódulo en pezón de largo tiempo de evolución. Actas Dermosifiliogr. 2015;106:501–502.



