


We present the case of a 40-year-old woman with no relevant medical history who presented with asymptomatic nodular-cystic lesions on a congenital alopecic plaque on the scalp. The lesions had developed slowly and progressively over the previous 5 years. The patient reported that her family physician had occasionally incised and drained some of the lesions. No cases of similar lesions were reported in her family history.
Physical ExaminationWe observed yellowish papules and skin-colored nodular-cystic lesions measuring 0.3 to 1cm in diameter that were soft on palpation and located on an alopecic plaque on the left frontotemporal region. The lesions extended to the left malar region (Fig. 1).
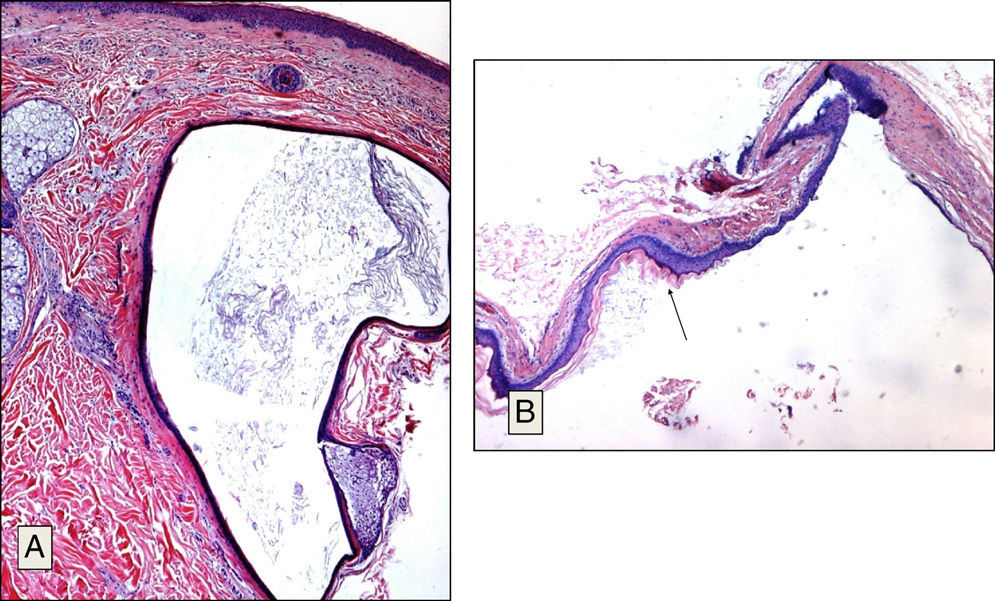
Histology
Several biopsies were taken from the area. Histologic findings revealed multilocular cystic epithelial tumors surrounded by a well-differentiated, flat epithelium with a crenulated lining that had an eosinophilic cuticle (Fig. 2, A and B). In addition, mature sebaceous glands were observed to be in close contact with the epithelium. Some of these glands opened into the lumen of the cyst.

What Is Your Diagnosis?
DiagnosisSteatocystoma multiplex (SM) on a congenital alopecic plaque on the scalp
Clinical Course and TreatmentSimple excision was performed on several of the larger lesions, and although the esthetic outcome was favorable, the patient rejected further treatment.
CommentSM is considered to result from hamartomatous malformations of the pilosebaceous unit. It is a rare condition that typically affects adolescents or young adults. Although it follows an autosomal dominant inheritance pattern, many sporadic cases have been described. Clinically, it consists of yellowish or skin-colored papules and nodules measuring 0.2 to 2cm in diameter that typically appear on the anterior aspect of the trunk and on the neck, axillas, thighs, and scrotum. Presentation on the scalp is rare and, unlike SM in more typical areas, it is not associated with an autosomal dominant inheritance pattern and appears in older individuals,1,2 as in our patient.
SM affecting the face and scalp has been classified into 3 types: a) a facial papular variant,3,4 b) sebocystomatosis,5 and c) lesions confined to the scalp.1,2,6,7
Only 12 cases of SM on the scalp have been described in the literature to date, and just 2 of these cases involved concurrent alopecic plaques. In 1996 Lee et al.5 reported a case of SM on the face and on a congenital alopecic plaque in the frontal region that they considered to be a clinical variant of this condition. The variant, which they called sebocystomatosis, had very similar clinical characteristics to those seen in our patient. The second published case of SM with concurrent alopecia on the scalp was described by Lee et al.8 in 2011. In that case the lesions appeared on an alopecic plaque caused by trichotillomania.
Some authors have described cases of SM associated with other disorders such as ichthyosis, koilonychia, pachyonychia congenita, acrokeratosis verruciformis of Hopf, hypertrophic lichen planus, hypohidrosis, hypothyroidism, hidradenitis suppurativa, and hypotrichosis.1 No associated conditions, however, have yet been described in patients with SM affecting the scalp only. Our patient had no other cutaneous manifestations or disorders.
Histologically, SM consists of cystic lesions that are empty, partially collapsed, folded, and covered with a wall formed by a stratified squamous epithelium lacking a granular layer and lined with a crenulated cuticle. Sebaceous gland lobules embedded in the cyst wall are also a very characteristic finding.
The clinical differential diagnosis typically includes eruptive vellus hair cysts, the histology of which shows cysts containing keratin and vellus hair surrounded by a thin wall comprised of several layers of squamous cells. As in SM, the sebaceous glands may form part of the cyst wall.
Other diagnoses to consider are epidermal cysts, milia cysts, neurofibromas, and xanthomas.
Although most SM lesions are asymptomatic, they may cause serious esthetic concern. Treatment with simple excision or drainage of cyst content may produce satisfactory results. In cases of inflamed lesions, treatment with locally injected corticosteroids, laser treatment, oral retinoids, and cryotherapy may be effective.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Fuentelsaz-del Barrio V, Parra Blanco V, Cieza Díaz D. Lesiones nódulo-quísticas sobre placa de alopecia congénita. Actas Dermosifiliogr. 2014;105:85–86.



