

Dermoscopy is mainly used to analyze pigmented lesions, but in recent years many studies have been published showing the usefulness of this tool in the evaluation of hair and scalp disorders.1 While most of the studies have focused on the characteristic dermoscopic features of different types of alopecia, in particular alopecia areata and androgenetic alopecia,1,2 there have been recent reports describing comma hairs as a dermoscopic marker of tinea capitis.3 Tinea capitis, a dermatophyte infection of the scalp, is still relatively common in routine dermatology practice. It mostly affects children, generally aged between 3 and 7 years,4 and trichoscopy may therefore be a very useful diagnostic tool in this setting because it is quick, reliable, inexpensive, and noninvasive.5 We describe 2 patients with tinea capitis and multiple comma hairs as a characteristic dermoscopic finding.
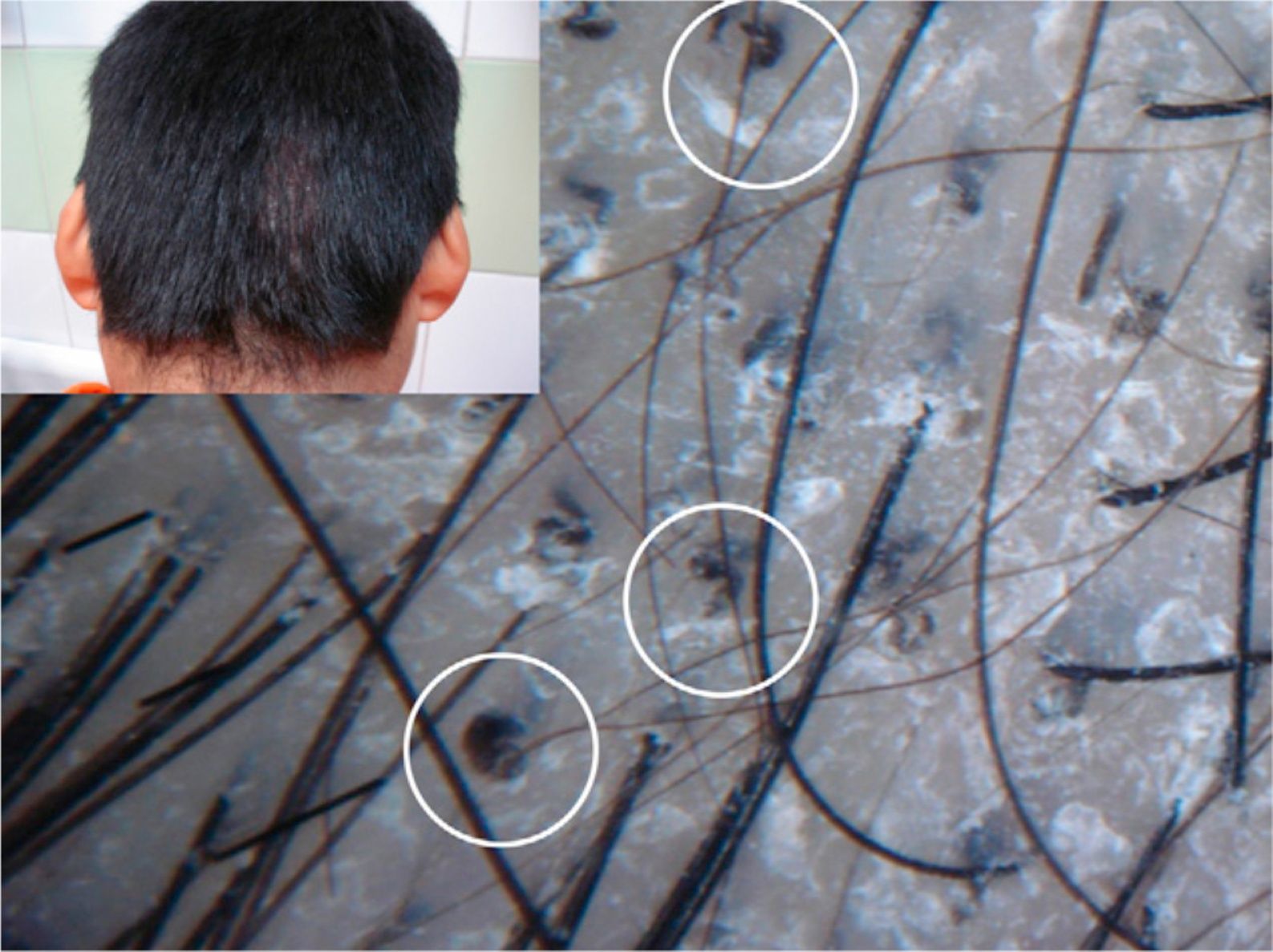
The first patient was a 9-year-old boy with a 10-month history of lesions on the scalp and face. The boy was originally from a village in Bolivia where he had had frequent contact with animals. Physical examination revealed fine whitish scale on the scalp and several plaques of alopecia with marked hair fragility on the hair pull test. The boy also had several erythematous, scaly plaques with irregular but well-defined borders on his face. There were no palpable lymph nodes in the lateral cervical chains. Dermoscopic evaluation of the hair structures showed multiple broken hairs as well as hairs with a characteristic comma-like shape (uniform thickness and color and marked distal angulation) (Fig. 1). Direct examination with potassium hydroxide and microbiological culture confirmed the presence of a zoophilic fungus, identified as Trichophyton verrucosum. The patient was administered oral griseofulvin at a dosage of 20mg/kg/d for 8 weeks. At follow-up 4 months later, the lesions had cleared completely, and there was no evidence of residual scarring alopecia.
 (handheld Dermlite II Pro dermoscope and Sony DSC-W55 camera, original magnification×40).")
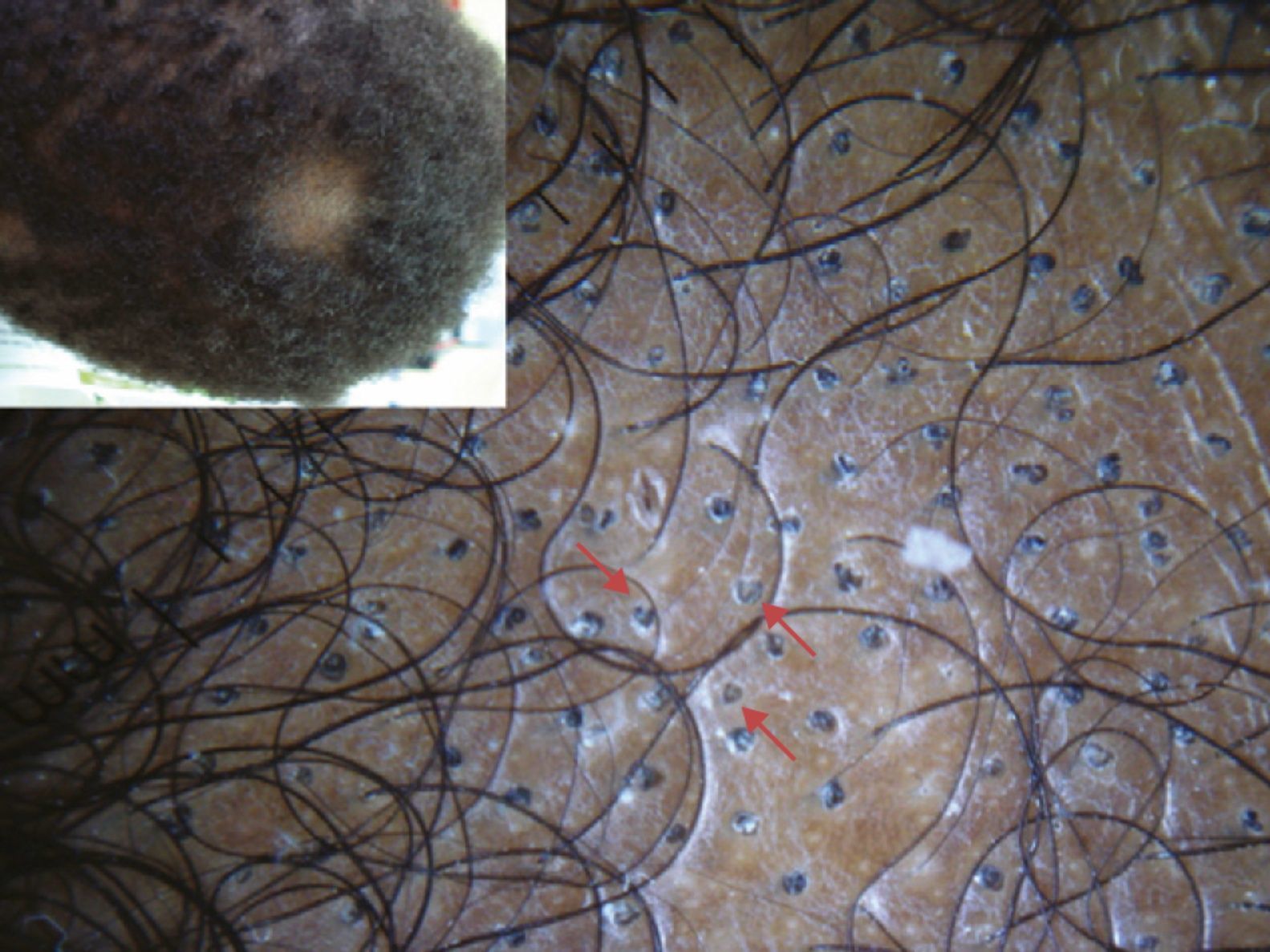
The second case is that of a 2-year-old boy from Senegal who was brought in for evaluation of several plaques of alopecia that had been present on the scalp for 6 months. The hair pull test was positive. On dermoscopic examination, there were multiple hairs with a characteristic comma shape (Fig. 2). Direct examination with potassium hydroxide was positive, but no fungi were isolated in the culture. The condition resolved completely with 8 weeks treatment of oral griseofulvin at 15mg/kg/d.
 are seen in the dermoscopic image (handheld Dermlite II Pro dermatoscope and Sony DSC-W55 camera, original magnification×20).")
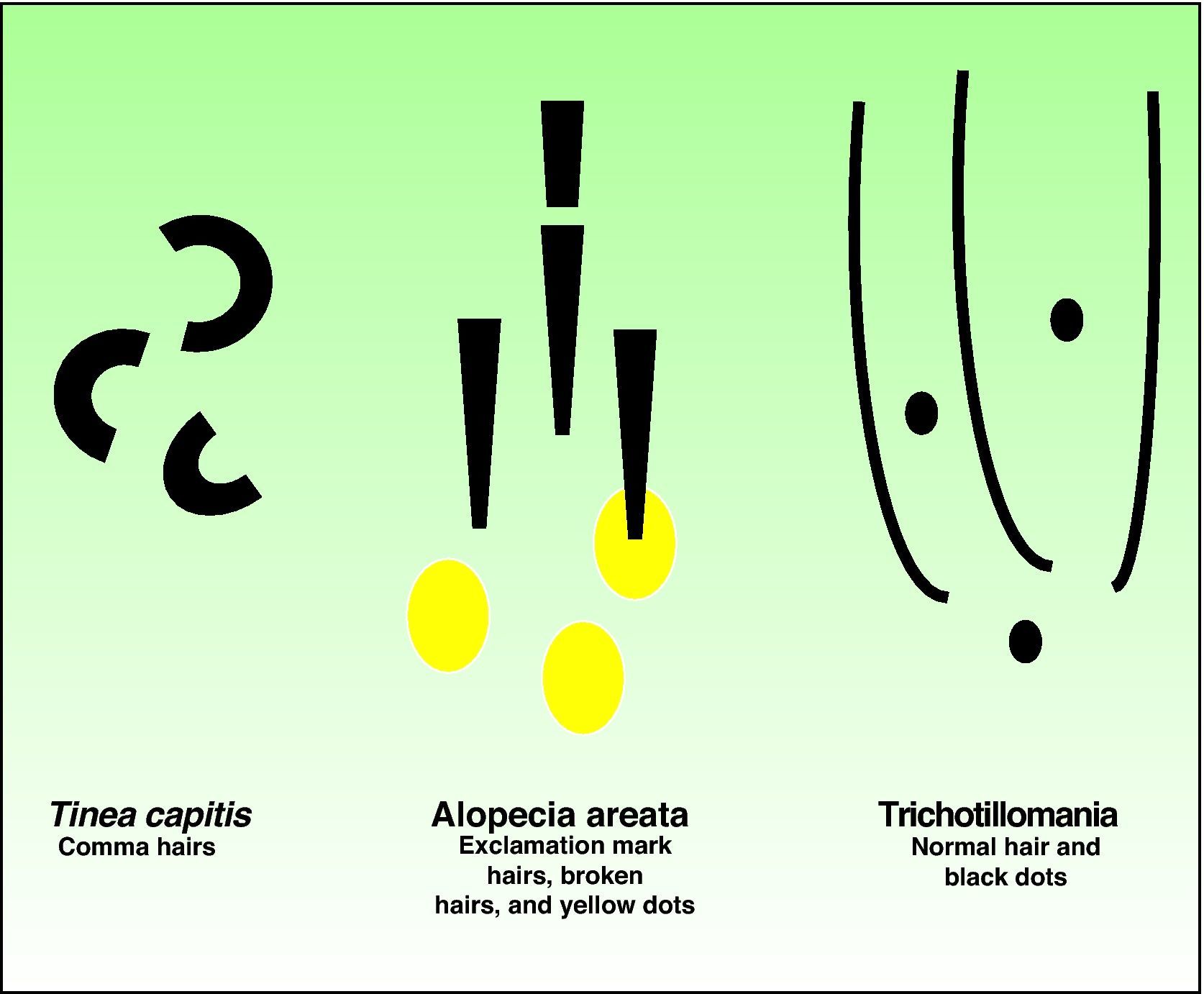
Tinea capitis is a common scalp infection in children. It is caused by different dermatophyte species of the genera Trichophyton and Microsporum and has a prevalence of approximately 1% in developed countries. The condition should be suspected in patients with a single or several small plaques of alopecia accompanied by broken hairs, desquamation, and itching.4 The differential diagnosis of hair loss in children should include tinea capitis, alopecia areata, traction alopecia, trichotillomania, and loose anagen syndrome, although in this last case, there is generally diffuse hair loss due to traction and an absence of itching and desquamation.6 Trichoscopy is also a very useful tool in many of these conditions and offers better diagnostic performance than simple clinical inspection as it can reveal distinctive features1,2,7 (Fig. 3). Characteristic findings in trichotillomania are hairs with a similar diameter, black dots, broken hairs of differing lengths, and coiled hairs (due to traction). In alopecia areata, dermoscopy shows smaller hair follicles, yellow dots, and exclamation mark hairs.7 In the 15 cases of tinea capitis evaluated by dermoscopy in the literature, the distinctive features were broken hairs and comma hairs. Comma hairs correspond to hair shafts that have ruptured because of the presence of multiple hyphae; they have a uniform thickness and color and marked distal angulation.3,5,8 Corkscrew hairs were recently proposed as a new dermoscopic marker of tinea capitis in black children, in whom clinical features can occasionally be more difficult to see.9 Of the 15 cases published to date of tinea capitis with comma hairs as a distinctive feature, 4 were caused by Microsporum canis, 1 by Microsporum langeronii, 4 by Trichophyton soudanense, 2 by Trichophyton tonsurans, and 1 by Trichophyton violaceum. The causative dermatophyte was not identified in 3 cases. None of the cases were due to T verrucosum, which was the fungus isolated in our first case.

In conclusion, we have described 2 cases of tinea capitis with comma hairs, a possible dermoscopic marker of this condition. We consider that trichoscopy is an effective, quick, cheap, and noninvasive tool that can aid in the diagnosis of tinea capitis.
We thank Dr Javier Pemán, from the Department of Microbiology at Hospital Universitari i Politècnic La Fe de Valencia, Spain for his contribution to the first case.
Hernández-Bel P, et al. Un nuevo marcador dermatoscópico de tinea capitis: «pelos en coma». Actas Dermosifiliogr. 2012;103:837-8.



