





Psoriasis is a chronic immunoinflammatory skin disease very frequent in the western world. Several authors have tried to calculate its prevalence in different regions, although most of them obtained the data from surveys and there are few publications from Mediterranean areas.
The objective of our study was to analyze the prevalence and severity of psoriasis in Lleida (a northeastern region in Spain), identify age and sex specific differences and compare our results with other European series.
Materials and methodsA joint database of primary care medicine and the dermatology department was obtained from the entire province of Lleida with epidemiological data and psoriasis diagnosis and treatment codification.
ResultsA corrected database was obtained with 398,701 individuals and 6,868 of them (1.72%) were coded with the diagnosis of psoriasis. The prevalence was significantly higher in men than in women (1.88% vs 1.56%, OR=1.21, 95% CI: 1.15-1.27). The highest prevalence of psoriasis was found in the 61-70 years group (2.90%) and psoriasis in population under 18 years of age was 0.30%. In our sample, 7.27% of the patients were classified as moderate-severe psoriasis (499/6,868).
ConclusionThis study reports the prevalence and severity of psoriasis in a large Mediterranean region sample, obtaining the information through a electronic database. This study reveals a lower prevalence of psoriasis compared to other European countries, and the proportion of severe psoriasis (based on treatment criteria) is lower than in other studies. We emphasize that these differences could probably due to genetic background, life style and diet.
La psoriasis es una enfermedad inmunoinflamatoria crónica de la piel muy frecuente en el mundo occidental. Muchos autores han intentado calcular su prevalencia en diversas regiones, aunque en la mayoría de los casos esta se ha obtenido mediante encuestas y existen escasas publicaciones procedentes del área mediterránea.
El objetivo de nuestro estudio era analizar la prevalencia y severidad de la psoriasis en Lleida (región del noreste de España), identificar diferencias en edad y sexo, y comparar nuestros resultados con otras series europeas.
Materiales y métodosSe obtuvo una base de datos conjunta entre medicina primaria y el departamento de dermatología de toda la provincia de Lleida con datos epidemiológicos, diagnóstico de psoriasis y codificación de tratamiento.
ResultadosLa base de datos final comprendía a 398.701 individuos y 6.868 de ellos (1,72%) fueron codificados con el diagnóstico de psoriasis. La prevalencia de psoriasis fue significativamente mayor en hombres que en mujeres (1,88 vs. 1,56%; OR=1,21; IC 95%: 1,15-1,27). La prevalencia más alta de psoriasis se encontró en el grupo de edad de los 61-70 años (2,90%) y la prevalencia de psoriasis en menores de 18 años fue del 0,30%. En nuestra población, el 7,27% de los pacientes fueron clasificados como psoriasis moderada-severa (499/6.868).
ConclusionesEste estudio reporta la prevalencia y severidad de la psoriasis en una muestra amplia de una región mediterránea, obteniendo la información mediante una base de datos electrónica. Además, se evidencia una prevalencia menor de psoriasis comparada con otros países europeos y una proporción de psoriasis severa (basado en criterios de tratamiento) menor que en otros estudios. Estas diferencias podrían deberse a factores genéticos, estilo de vida y dieta.
Psoriasis is a chronic immune-inflammatory cutaneous disease affecting 1-3% of the world population,1,2 corresponding to about 125 million individuals.3 In Spain, the estimated prevalence of psoriasis was 1.4-2.7% through two telephonic surveys.4,5 In addition, it has a significant impact on self-esteem and quality of life, and patients with moderate to severe psoriasis report a similar quality of life to heart failure or breast cancer.6
A great proportion of the studies performed to calculate the prevalence of diseases such as psoriasis have been conducted by means of surveys, studying only a portion of the population that is significant enough. In addition, the geographic zone may modify psoriasis prevalence 7and there are not many population-based studies of psoriasis epidemiology in Mediterranean areas, where population diet or habits could play an important role.8 The objective of this study is to know the prevalence and severity of psoriasis (globally and by subgroups) through the analysis of a computerized clinical history (eCAP) that collects all the inhabitants of Lleida, a province located in the northeast of Spain, in Catalonia.
Materials and methodsThis is an observational and cross-sectional population study on electronic medical records (eCAP and SAP) of residents in the province of Lleida.
The Primary Care computerized register was obtained from the clinical station of ECAP, which covers the province of Lleida with the exception of the Solsonès area. This database is active since 2003 and includes approximately 1,000,000 people who have contacted with primary care services since then. Dermatology department data was obtained from SAP, a medical electronic register used by Hospital Arnau de Vilanova, the only hospital in the province of Lleida with a dermatology department. It is active since 2010. This databases did not include those individuals who had never been evaluated in the public health system.
Information from these two databases was obtained (since its beginning to June 2016) and merged. Only items relevant to the study were extracted (sex, age, height, weight, diagnosis of psoriasis and drugs used for the treatment of this disease). Once obtained this database, those individuals who did not belong to this area were discarded. From the resulting database, duplications were eliminated and the records with the diagnosis of cutaneous psoriasis (DL20, 696.1) were selected using the ICD-10 international classification. Information from prescribed drugs was obtained since 2005 (ECAP program) and 2010 (SAP program). This information was then combined and compared with the Catalan national registry of prescriptions.
In the final database, each individual presented: an anonymized identification once interacted with the hospital database, age at the time of the study, whether there was available information from the hospital or not (with their values), sex and the rest of the variables requested in the study and mentioned before. All the data was safely stored and this anonymized identification allowed to review or to verify the information of each register if it were necessary.
Due to the possibility of patients with psoriasis who had not been registered in the health system, we decided to add to the group of psoriasis those who had been treated with topical vitamin D analogues (alone or combined with topical betamethasone) and those who had received oral acitretin.
The anonymized database was captured and analysed with SPSS v24.0 software (IBM Corporation, Armonk, NY, USA). Comparisons of proportions and ranges of variables between different groups were performed by chi-square, Student's t-test or one-way ANOVA as appropriate. The selected P value for considering differences as statistically significant in all analyses was P<0.05.
We defined moderate-severe psoriasis when the patient had registered history of treatment with narrowband UVB (NB-UVB), psoralen and ultraviolet A (PUVA), traditional systemic drugs (acitretin, methotrexate or cyclosporine) or biological therapy (infliximab, etanercept, adalimumab, ustekinumab, secukinumab or ixekizumab), labeling the rest as mild psoriasis. This method has been used previously by some authors.9 The study was approved by the “Hospital Arnau de Vilanova de Lleida ethics committee”.
ResultsThe joint hospital / primary care database collected a total of 398,860 records. After excluding inconsistencies, as well as lack of any of these data, the resulting corrected database consisted of 398,701 individuals. The mean age was 42.34 (median 42.00, interquartile range 25.00-59.00 years) and the percentage of males was 50.66% (201,977 males). Of these, 72,230 individuals were under 18 years of age (18.12% of the total sample) (Table 1).
Population characteristics.
In the initial database we found 6,556 records with the diagnosis of psoriasis. We added to this group 298 patients who had been treated with topical vitamin D analogues (alone or combined with topical betamethasone) and 14 who had received oral acitretin and had not been previously registered as psoriatic, resulting in 6,868 patients (1.72% of the population). Males with psoriasis in our sample (3,799/6,868 individuals) accounted for 55.31% of the total, with a male prevalence of psoriasis of 1.88% (3,799/201,977). On the other hand, the prevalence of psoriasis in women was 1.56% (3,069/196,724). The male sex was a factor associated with the risk of psoriasis (OR=1.21, 95% IC: 1.15-1.27).
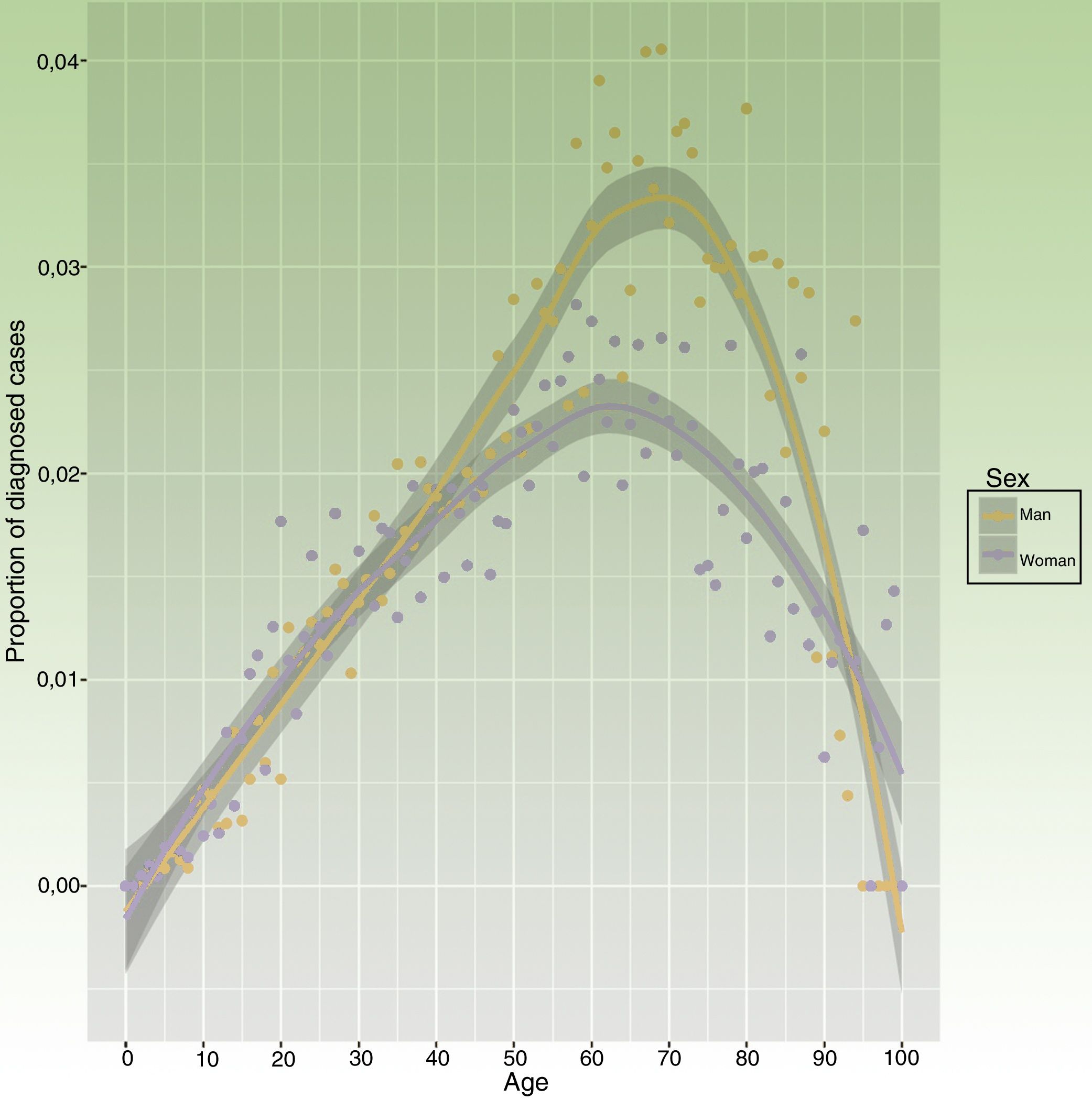
The mean age of the psoriasis group was higher than the general population (52.08 vs 42.34 years, p<0.001). There were 217 individuals younger than 18 years (217/6,867), which represents a 3.16% of patients with psoriasis and 0.29% of those younger than 18 years) (Table 1). Psoriasis prevalence in females younger than 18 years was greater than in males without statistical signification (0.33% vs 0.27%, OR=1.210, 95% IC: 0.926-1.581). The age group with the highest absolute number of patients with psoriasis was between 51 and 60 years (1,350/6,868 individuals, and a 19.66% of the psoriasis group). However, highest prevalence of psoriasis was in the 61-70 age group (1,122/38,740 individuals), representing a 2.90% of this group (Table 2, Fig. 1). There were 499 patients whose psoriasis was classified as moderate-severe (7.27% of patients with psoriasis).
Population distribution in relation to age and sex.
| Age group | General population | Non-psoriasis group | Psoriasis group | |||
|---|---|---|---|---|---|---|
| Men n (%) | Women n (%) | Men n (%) | Women n (%) | Men n (%) | Womenn (%) | |
| 0-10 | 23,327 (11,55%) | 22,276 (11,33%) | 23,293 (11,75%) | 22,245 (11,49%) | 34 (0,89%) | 31(1,01%) |
| 11-20 | 19,442 (9,63%) | 18,158 (9,23%) | 19,335 (9,76%) | 18,012 (9,30%) | 107 (2,82%) | 146 (4,76%) |
| 21-30 | 21,246 (10,52%) | 20,620 (10,48%) | 20,976 (10,58%) | 20,347 (10,51%) | 270 (7,11%) | 273 (8,90%) |
| 31-40 | 33,797 (16,73%) | 29,475 (14,99%) | 33,200 (16,75%) | 28,994 (14,97%) | 597 (15,71%) | 481 (15,68) |
| 41-50 | 34,940 (17,30%) | 29,941 (15,22%) | 34,208 (17,26%) | 29,405 (15,19%) | 732 (19,27%) | 536 (17,47%) |
| 51-60 | 27,911 (13,82%) | 25,467 (12,95%) | 27,156 (13,70%) | 24,872 (12,85%) | 755 (19,87%) | 595 (19,39%) |
| 61-70 | 19,051 (9,43%) | 19,689 (10,01%) | 18,392 (9,28%) | 19,226 (9,93%) | 659 (17,35%) | 463 (15,09%) |
| 71-80 | 12,481 (6,18%) | 15,226 (7,74%) | 12,070 (6,09%) | 14,923 (7,71%) | 411 (10,82%) | 303 (9,88%) |
| 81-90 | 8,489 (4,20%) | 12,957 (6,59%) | 8,267 (4,17%) | 12,747 (6,58%) | 222 (5,84%) | 210 (6,84%) |
| 91or more | 1,293 (0,64%) | 2,878 (1,46%) | 1,281 (0,65%) | 2,848 (1,47%) | 12 (0,32%) | 30(0,98%) |
The prevalence of psoriasis in the province of Lleida, Spain (1.72%) is within the range of previous studies in Spain (1.43% in 2001 4and 2.31% in 20135), with a studied population of 12,938 and 12,711 people respectively. It should be noted that the method of registration was by telephone survey and not a medical database. As our study, there are other European studies that evaluated the prevalence of psoriasis through databases (Table 3), such as those of Springate et. al.10 in the United Kingdom and Radtke et. al.11 in Germany, with a prevalence of 2.8% and 2.78% respectively. Since information was extracted through similar methodologies, prevalence differences in our study may be due to population characteristics as well as environmental and dietary characteristics.8 In relation to other studies carried out in European countries, there is a great variety in the prevalence data. The lowest (0.73%) was recorded in Scotland 12and the highest (11.43%) in Norway,13 quite high data in relation to the largest proportion of population studies (1-3%), which could be due to the Norwegian study was conducted in a closed community region and through interviews and that the diagnosis of psoriasis was reported by the same patient and was not a medical diagnosis. Focusing on Mediterranean countries, most recent and trustworthy data of prevalence of psoriasis were obtained in Italy (2.9%) 14and France (5.2%) 15(Table 3). Prevalence estimated in our Spanish study is similar to the data obtained in Italy, which suggests cultural and environmental factors are relevant in psoriasis prevalence. However, differences between Mediterranean countries could be due to methodological variations (surveys instead of databases).
Global prevalence and in variousgropusof psoriasis in some European relevant previous studies.
| Study | Country | Year | Diagnosis method | Population(n) | Age | Global psoriasisprevalence(%) | Men prevalence(%) | Women prevalence(%) | Prevalence under18years (%) |
|---|---|---|---|---|---|---|---|---|---|
| SaracenoR et. al. (2008)14 | Italy | 2006 | Survey | 4,109 | All ages | 2.9 | - | - | - |
| WolkensteinP et. al. (2009)15 | France | 2005 | Survey | 6,887 | 15+ | 5.2 | - | - | - |
| SeminaraNM et. al. (2011)22 | United Kingdom | 2009 | Database+ survey | 7,520,293 | All ages | 1.9 | 1.8 | 1.9 | 0.40 |
| FerrandizC et. al. (2014)5 | Spain | 2013 | Telephone survey | 12,711 | All ages | 2.3 | 2.7% | 1,9 | 0,5 (< 16yearsold) |
| CantaruttiA et. al. (2015)16 | Italy | 2006-2012 | Survey | 145,233 | 0-14 | - | - | - | 0.22 (2012) |
| RadtkeMA et. al. (2016)11 | Germany | 2009 | Database | 1,349,671 | 18+ | 2.78 | 2.94 | 2.59 | - |
| SpringateDA et. al. (2017)10 | United Kingdom | 1999-2013 | Database | 15,436,637 (2013) | All ages | 2.8 | 2.81% | 2.83 | - |
The mean age of the general population under study was 42.34 years (interquartile range 25.00-59.00 years) and interestingly, among the group of patients with psoriasis, this mean age increased to 52.08 years, reflecting that this disease usually appears from adolescence. Regarding the distribution of patients with psoriasis by age subgroups, the highest percentage of psoriasis patients was observed in the 51-60 age group (19.66% of the psoriasis population) (Table 2), and the maximum prevalence was observed in the 61-70 age group (2.90%). These data are comparable to those of most studies, where there is an increase in the prevalence of psoriasis directly proportional to age up to 60-70 years, when the frequency of this disease decreases5,13(Table 3). These results concur with the fact that it is a chronic disease and patients who start this disease at earlier ages accumulate over the years. On the other hand, there are some studies in which there is a first peak of prevalence in the subgroup of 20 to 30 years old patients,4,10 a fact that not has been observed in our study.
The percentage of psoriasis in population under 18 was 0.30%, which corresponds to 3.16% of the psoriatic population (Table 1). These data are similar to those published by Cantarutti et. al. in Italy (0.22%) 16(Table 3) and Augustin et. al. in Germany (0.45%).17 There is a study of childhood psoriasis in Italy where they estimate a prevalence in children between 12 and 17 years of age of 2.1% with an association between the diagnosis of atopic dermatitis and psoriasis.18 The authors suggest that this higher prevalence of psoriasis in Italian children could be the possible misdiagnosis of eczema in children as psoriasis lesions. Similarly, the prevalence of childhood psoriasis in European countries is higher than other published African or Asian population studies,19,20 which is comparable to adult psoriasis. Even though these authors do not hypothesize any reason for these results, environment and dietary differences in these areas could be involved.
Male sex was a factor associated with the risk of psoriasis (1.88% vs 1.56%, OR: 1.21, 95% IC: 1.15-1.27) (Table 1). This higher proportion of men is also seen in other European studies such as Ferrándiz et. al. in Spain 5(Table 3) (2.4% vs 1.9%) and Radtke et. al. in Germany 11(Table 3) (2.90% vs. 2.59%). Other studies show a higher prevalence of psoriasis in women, such as Stern et. al. in the US (2.5% in women vs. 1.9 in men),21 whereas two UK studies found no significant difference between sexes 22,23(Table 3). In the study of Augustin et. al. which included German children, psoriasis was more frequent in women (0.76% vs. 0.66).24 Prevalence of psoriasis in children in our study was smaller, even though we also obtained a larger proportion of psoriasis in females (0.33% vs 0.27%, OR=1.210, 95% IC: 0.926-1.581) without statistical signification. Since there is no consensus about sex and psoriasis association among publication results, it might be interesting to elucidate which factors could interfere in these found differences.
Nowadays, there are few published studies which differentiate between mild psoriasis prevalence and moderate-severe disease. In our population, 499 patients (7.27% of all patients with psoriasis) had a psoriasis classified as moderate-severe), a much lower prevalence than other series such as Takeshita et. al. in United States (27.3%) 9and Yeung et. al. in United Kingdom (38.2%).25 A possible hypothesis may be an underestimation of the percentage of moderate-severe psoriasis using the systemic treatment as criteria. Nonetheless, psoriasis severity scales (BSA or PASI) are not equally available for all patients with psoriasis since this is not usually measured in patients who are followed by primary care, and we considered results obtained by this method could not be trustworthy. Another hypothesis could be the under-treatment of moderate to severe psoriasis with topical medications in a country with a sunny climate.26 In addition, other environmental components such as diet 8could have a protective effect and might avoid the worsening of many patients with psoriasis.
Limitations of the studySince this is a cross-sectional population study, there may be an underreporting in the database. Our database was obtained from Primary Care and the Dermatology department and those patients who had never been evaluated in the public health system were not registered in our database.
Furthermore, some patients might have only been visited by general practitioners, and there could be a certain proportion of misdiagnosed cases. Our classification of psoriasis severity according to the prescribed treatment is not the most adequate and a classification according to BSA or PASI could be more suitable. However, since the vast majority of psoriasis patients in our study did not have BSA or PASI (most of them are only followed by general practitioners and these values are not usually registered), we decided to differentiate patients according to the prescribed treatment. In our study, individuals who had received acitretin and topical vitamin D analogues were added to the psoriasis group since these drugs are usually prescribed to psoriatic patients. This was done with the intention of adding possible patients not coded for psoriasis but who were under treatment. It is important to emphasize that there may be a small percentage that could not have this pathology and this might produce a bias in the results.
Since in this population there is only one center that prescribes systemic or biological treatments for patients with psoriasis, the criteria for starting this type of medication could be different from other centers.
ConclusionOur study reflects the relatively lower prevalence and severity of psoriasis in the general population compared to most of the western world studies and its association to male gender. The variations between different populations of the world make it interesting to carry out the same studies in distinct regions, in order to better understand the disease and the factors that may be involved. Methodological issues could explain some of the differences obtained in our manuscript and subsequent studies would be needed to compare interregional data differences and at the same time corroborate or question psoriasis associations with other genetic or epidemiological factors.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Fernández-Armenteros JM, Gómez-Arbonés X, Buti-Solé M, Betriu-Bars A, Sanmartin-Novell V, Ortega-Bravo M, et al. Características epidemiológicas de la psoriasis. Un estudio poblacional. Actas Dermosifiliogr. 2019;110:385–392.


