
Previous studies in Spain have shown that the foreign and immigrant populations can have different diseases to Spanish-born individuals. However, no comparative study has specifically investigated foreign children in Spain.
Material and methodsThe objective of the study was to compare skin diseases in foreign children with those in children born in Spain of Spanish parents. We included all patients under 15 years of age who were seen in our dermatology department between January 2007 and December 2007.
ResultsDuring the study period, 3108 pediatric patients were seen in the dermatology department. Of these, 2661 (85.6%) were Spanish and 447 (14.3%) were foreigners. Foreign children sought medical care more often (11.4%) than Spanish children (6%) (P<.001) and made less use of the specialist outpatient clinic (59.6% vs 68.8% [P<.001]) and more use of emergency care. Complaints observed more frequently in the foreign children were scabies (adjusted odds ratio [aOR], 10.6; 95% CI, 4.71-24.10), arthropod bites (aOR, 2.80; 95% CI, 1.14-6.87), hypopigmentation (aOR, 2.61; 95% CI, 1.06-6.44), and atopic dermatitis (aOR, 1.65; 95% CI, 1.19-2.31). Melanocytic nevus was observed more frequently in Spanish children (aOR, .50; 95% CI, .30-.83).
ConclusionsDifferences between children born in Spain of Spanish parents and foreign children were found for type of visit and frequency of skin diseases.
En estudios anteriores realizados en nuestro país se ha constatado que la población extranjera e inmigrante puede tener enfermedades diferentes a la población autóctona. Sin embargo, no existe ningún estudio diseñado sobre población infantil inmigrante en España.
Material y métodosEl objetivo de este estudio fue el de analizar las dermatosis de la población inmigrante infantil y compararlas con la población autóctona. Se incluyó a todos los pacientes menores de 15 años que fueron atendidos en la sección de dermatología entre enero de 2007 y diciembre de 2007.
ResultadosDurante el periodo de estudio se registraron 3.108 episodios de consulta en población pediátrica, de ellos 2.661 (85,6%) correspondieron a población autóctona y 447 (14,3%) a población inmigrante. La población infantil inmigrante acudió a la consulta (11,4%) más que la población autóctona (6%) (p<0,001), consultando menos en la consulta ambulatoria especializada (59,6 vs 68,8%) (p<0,001) y más por urgencias. La escabiosis (ORa: 10,6; IC 95%: 4,71-24,10), las picaduras de artrópodos (ORa: 2,80; IC 95%: 1,14-6,87), la hipopigmentación (ORa: 2,61; IC 95%: 1,06-6,44) y la dermatitis atópica (ORa: 1,65; IC 95%: 1,19-2,31) fueron más frecuentes en la población inmigrante. El nevus melanocítico fue más frecuente en la población autóctona (ORa: 0,50; IC 95%: 0,30-0,83).
ConclusionesExisten diferencias tanto en la forma de consultar como en la frecuencia de las dermatosis presentadas en la población infantil autóctona e inmigrante.
Immigration is a dynamic and inevitable process. Since 1999, the foreign population has increased exponentially in size. Between 1998 and 2012, the number of foreigners registered as residents in Spain increased more than 6-fold from 637 058 to 5.7 million.1
Although the recent economic crisis has forced many foreigners to leave Spain, the foreign population still accounts for 12% of the census population (as of January 2012).1 Children account for 14.5% of registered foreigners, that is, a proportion similar to the population of Spanish origin (15%), although this figure does not include children of foreigners settled in Spain, for whom no census data are available.
The new sociodemographic realities in our country demand an analysis of the needs and priorities at all levels of care.2 The foreign pediatric population may have a different prevalence of certain diseases compared to the Spanish population,3,4 as demonstrated in Spanish5,6 and international studies.7,8 Likewise, several Spanish studies have investigated the demand generated in dermatology clinics by foreign patients.9–11 However, there are no studies on skin diseases in the foreign pediatric population in Spain. We therefore thought it of interest to assess the skin diseases present in the foreign pediatric population and compare them with the Spanish population.
The objective of the study was to analyze skin diseases in foreign children and compare them with those in Spanish children and to evaluate certain socioepidemiologic variables and the frequency of visits to the different care settings within the department.
Patients and MethodsIn this prospective, descriptive, and analytical study, patients had to be under 15 years of age and attended by a dermatologist between January and December 2007.
The study covered the care activity in the dermatology department of the Nineteenth Health District of the Valencian Community and included all outpatient and hospital clinics, as well as surgery appointments and walk-in visits.
Patients were divided into 4 categories: 1) Spanish patients (born in Spain of Spanish parents); 2) children of foreigners (born in Spain of at least one parent born outside Spain); 3) foreign children (born outside Spain); and 4) adopted children. Patients in the latter 3 categories were considered foreign patients for the purposes of this study.
VariablesData were collected using a case report form filled out by the physician (attending and resident physicians). The outcome variable was the dermatologic diagnosis or skin disease, classified according to the International Classification of Diseases (ICD) version 9, adapted to dermatology.12
Skin diseases were grouped into 8 diagnostic categories: infectious diseases, erythematous-desquamative lesions, melanocytic lesions, tumors, skin appendage diseases, pigmentation abnormalities, lesions of exogenous origin, and others (including genodermatosis, malformations, other inflammatory conditions, neonatal conditions, and connective tissue disorders).
Independent variables were collected at all visits. These variables included 3 types:1) epidemiologic variables (age, sex, skin type [white, black, native American, Asian Indian, Arabic, and Oriental]) and type of patient (foreigner, child of foreigner, or adopted); 2) sociodemographic variables: country of origin of the child and/or parents (for children of foreigners) and geographic area (Latin America, North Africa, Sub-Saharan Africa, Eastern Europe [that is, those countries not in the 12 founder states of the European Union], and Asia), number of siblings and cohabiters in the home and physical activity; and 3) healthcare variables such as setting within the dermatology department in which the patient was seen (specialized outpatient clinic, hospital clinic, hospital admission, walk-in visit to the dermatology clinic, and surgery), type of visit (first visit or follow-up visit), and month and year.
Statistical AnalysisThe data were analyzed using the SPSS statistical program, version 12.0 (SPSS Inc., Chicago, Illinois, USA). For comparison of continuous variables with a normal distribution, the Student t test was used for 2 independent samples. For comparison of categoric variables, the χ2 test with the Yates correction was used. The Fisher exact test was used in cases that did not meet the conditions for the χ2 test. The size of the association of the skin diseases was assessed using the odds ratio (OR) with the corresponding 95% confidence interval (CI). The size of the association of the type of population with skin diseases and diagnostic category was adjusted for age and sex to yield the adjusted odds ratio (aOR), calculated using logistic regression by means of the method of maximum unconditional probability. P values less than .05 were considered significant.
ResultsHealthcare Usage Data for Foreign ChildrenDuring the study period, 3108 pediatric patients were seen in the dermatology department. Of these, 2661 (85.6%) were Spanish and 447 (14.3%) were foreign children (as defined in the methods). Visits were mainly in an outpatient setting (68.8%) or a hospital setting (22.5%).
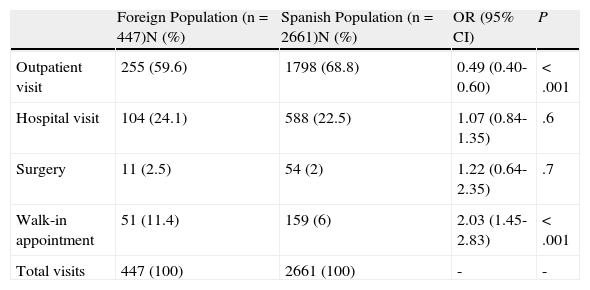
Comparison of Type of Visit With Spanish ChildrenTable 1 shows type of visits in which foreign and Spanish children were seen. Of note is that foreign children were seen twice as often in walk-in appointments (11.4%) compared to Spanish children (6%) (P<.001) and that foreign children made less use, in relative terms, of specialist outpatient clinics (59.6% vs 68.8%) (P<.001).
Visits by Foreign and Spanish Children.
| Foreign Population (n=447)N (%) | Spanish Population (n=2661)N (%) | OR (95% CI) | P | |
| Outpatient visit | 255 (59.6) | 1798 (68.8) | 0.49 (0.40-0.60) | <.001 |
| Hospital visit | 104 (24.1) | 588 (22.5) | 1.07 (0.84-1.35) | .6 |
| Surgery | 11 (2.5) | 54 (2) | 1.22 (0.64-2.35) | .7 |
| Walk-in appointment | 51 (11.4) | 159 (6) | 2.03 (1.45-2.83) | <.001 |
| Total visits | 447 (100) | 2661 (100) | - | - |
Abbreviation: OR, odds ratio.
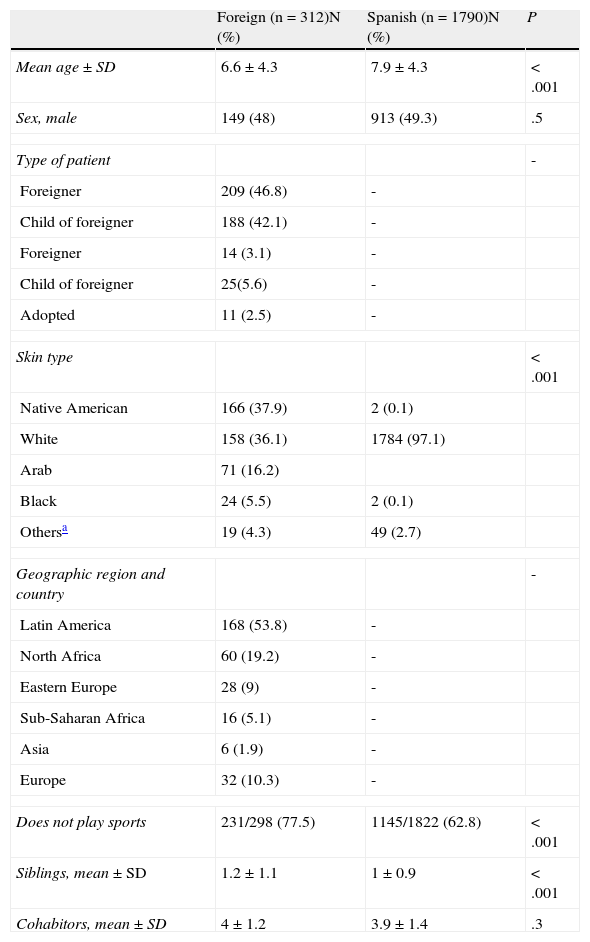
During the study period, 312 foreign children were attended in 477 visits. Table 2 describes the characteristics of the foreign children and their region and country of origin. Of these, 49.7% had been born outside Spain (46.8% were immigrants and 3.1% were foreigners from countries with equal or higher income per capita compared to Spain), 42.1% were children of foreigners, and 2.5% were adopted. Patients of Latin American origin (53.8%) were the ones who were seen most frequently in our department, followed by patients of North African origin (19.2%).
Epidemiologic Characteristics and Geographic Region of Origin of Immigrant and Foreign Children.
| Foreign (n=312)N (%) | Spanish (n=1790)N (%) | P | |
| Mean age ±SD | 6.6±4.3 | 7.9±4.3 | <.001 |
| Sex, male | 149 (48) | 913 (49.3) | .5 |
| Type of patient | - | ||
| Foreigner | 209 (46.8) | - | |
| Child of foreigner | 188 (42.1) | - | |
| Foreigner | 14 (3.1) | - | |
| Child of foreigner | 25(5.6) | - | |
| Adopted | 11 (2.5) | - | |
| Skin type | <.001 | ||
| Native American | 166 (37.9) | 2 (0.1) | |
| White | 158 (36.1) | 1784 (97.1) | |
| Arab | 71 (16.2) | ||
| Black | 24 (5.5) | 2 (0.1) | |
| Othersa | 19 (4.3) | 49 (2.7) | |
| Geographic region and country | - | ||
| Latin America | 168 (53.8) | - | |
| North Africa | 60 (19.2) | - | |
| Eastern Europe | 28 (9) | - | |
| Sub-Saharan Africa | 16 (5.1) | - | |
| Asia | 6 (1.9) | - | |
| Europe | 32 (10.3) | - | |
| Does not play sports | 231/298 (77.5) | 1145/1822 (62.8) | <.001 |
| Siblings, mean±SD | 1.2±1.1 | 1±0.9 | <.001 |
| Cohabitors, mean±SD | 4±1.2 | 3.9±1.4 | .3 |
The age of foreign children was slightly lower (mean, 6.7 years vs 7.9 years) compared to Spanish children (P<.001). No differences in terms of sex or number of cohabiters were observed, although foreign children did have more siblings compared to Spanish children (1.2[1.1] vs 1 [0.9]; P<.001) and fewer practiced sport (22.5% vs 37.2%; P<.001) (Table 2).
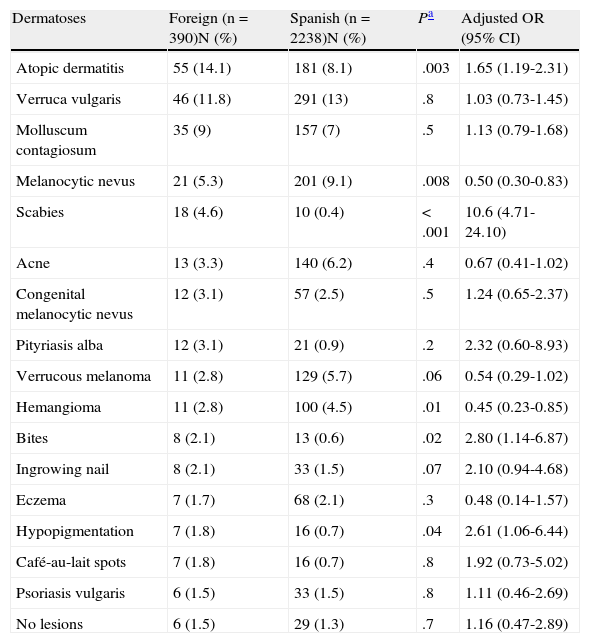
Skin Diseases in Foreign ChildrenThe 312 foreign children attended 447 visits and 503 diagnoses were made (mean of 1.12 diagnoses per visit). Of these diagnoses, 390 were absolute diagnoses (repeat diagnoses at follow-up visits were excluded). The 10 most frequently reported skin diseases accounted for 59% of all diagnosed cases. The most frequent condition was atopic dermatitis (14.1%) followed by extragenital warts (11.8%), molluscum contagiosum (9%), scabies (4.6%), and melanocytic nevus (4.4%) (Table 3).
Main Skin Diseases in the Foreign Population and Comparison with the Spanish Population.
| Dermatoses | Foreign (n=390)N (%) | Spanish (n=2238)N (%) | Pa | Adjusted OR (95% CI) |
| Atopic dermatitis | 55 (14.1) | 181 (8.1) | .003 | 1.65 (1.19-2.31) |
| Verruca vulgaris | 46 (11.8) | 291 (13) | .8 | 1.03 (0.73-1.45) |
| Molluscum contagiosum | 35 (9) | 157 (7) | .5 | 1.13 (0.79-1.68) |
| Melanocytic nevus | 21 (5.3) | 201 (9.1) | .008 | 0.50 (0.30-0.83) |
| Scabies | 18 (4.6) | 10 (0.4) | <.001 | 10.6 (4.71-24.10) |
| Acne | 13 (3.3) | 140 (6.2) | .4 | 0.67 (0.41-1.02) |
| Congenital melanocytic nevus | 12 (3.1) | 57 (2.5) | .5 | 1.24 (0.65-2.37) |
| Pityriasis alba | 12 (3.1) | 21 (0.9) | .2 | 2.32 (0.60-8.93) |
| Verrucous melanoma | 11 (2.8) | 129 (5.7) | .06 | 0.54 (0.29-1.02) |
| Hemangioma | 11 (2.8) | 100 (4.5) | .01 | 0.45 (0.23-0.85) |
| Bites | 8 (2.1) | 13 (0.6) | .02 | 2.80 (1.14-6.87) |
| Ingrowing nail | 8 (2.1) | 33 (1.5) | .07 | 2.10 (0.94-4.68) |
| Eczema | 7 (1.7) | 68 (2.1) | .3 | 0.48 (0.14-1.57) |
| Hypopigmentation | 7 (1.8) | 16 (0.7) | .04 | 2.61 (1.06-6.44) |
| Café-au-lait spots | 7 (1.8) | 16 (0.7) | .8 | 1.92 (0.73-5.02) |
| Psoriasis vulgaris | 6 (1.5) | 33 (1.5) | .8 | 1.11 (0.46-2.69) |
| No lesions | 6 (1.5) | 29 (1.3) | .7 | 1.16 (0.47-2.89) |
Abbreviation: OR, odds ratio.
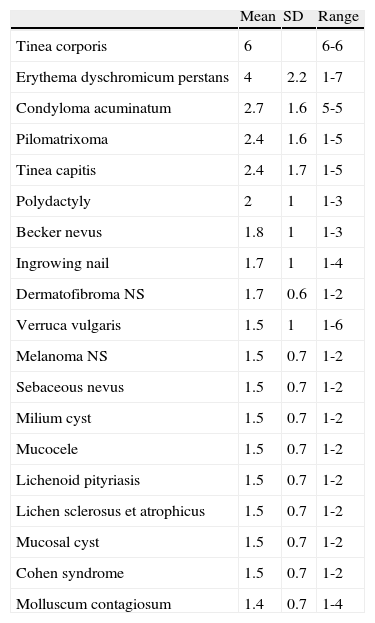
The mean (SD) number of follow-up visits per diagnosis was 1.37 (0.89) (range, 1-7). The skin diseases that required the most number of follow-up visits were tinea corporis (mean of 6) and erythema dyschromicum perstans (mean of 4), followed by condyloma acuminatum, pilomatrixoma, and tinea capitis (Table 4).
Follow-up Visits in Foreign Children by Skin Disease.
| Mean | SD | Range | |
| Tinea corporis | 6 | 6-6 | |
| Erythema dyschromicum perstans | 4 | 2.2 | 1-7 |
| Condyloma acuminatum | 2.7 | 1.6 | 5-5 |
| Pilomatrixoma | 2.4 | 1.6 | 1-5 |
| Tinea capitis | 2.4 | 1.7 | 1-5 |
| Polydactyly | 2 | 1 | 1-3 |
| Becker nevus | 1.8 | 1 | 1-3 |
| Ingrowing nail | 1.7 | 1 | 1-4 |
| Dermatofibroma NS | 1.7 | 0.6 | 1-2 |
| Verruca vulgaris | 1.5 | 1 | 1-6 |
| Melanoma NS | 1.5 | 0.7 | 1-2 |
| Sebaceous nevus | 1.5 | 0.7 | 1-2 |
| Milium cyst | 1.5 | 0.7 | 1-2 |
| Mucocele | 1.5 | 0.7 | 1-2 |
| Lichenoid pityriasis | 1.5 | 0.7 | 1-2 |
| Lichen sclerosus et atrophicus | 1.5 | 0.7 | 1-2 |
| Mucosal cyst | 1.5 | 0.7 | 1-2 |
| Cohen syndrome | 1.5 | 0.7 | 1-2 |
| Molluscum contagiosum | 1.4 | 0.7 | 1-4 |
Abbreviation: NS, not specified
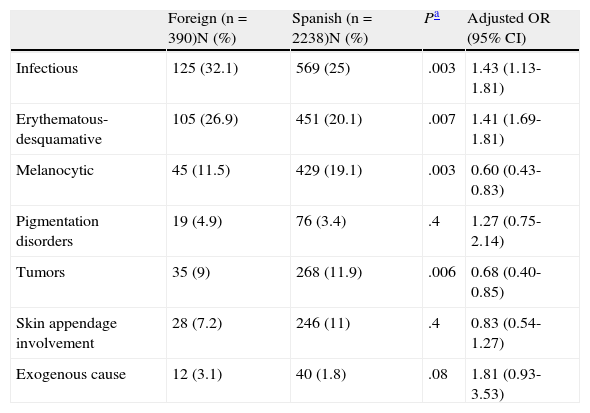
Within the diagnostic categories, infectious diseases and erythematous-desquamative diseases were the most frequently reported (32.1% and 26.9%, respectively). Along with the third most common category, melanocytic lesions (11.5%), these accounted for 70.5% of all processes (Table 5).
Diagnostic Categories for Spanish Population and Foreign Population.
| Foreign (n=390)N (%) | Spanish (n=2238)N (%) | Pa | Adjusted OR (95% CI) | |
| Infectious | 125 (32.1) | 569 (25) | .003 | 1.43 (1.13-1.81) |
| Erythematous-desquamative | 105 (26.9) | 451 (20.1) | .007 | 1.41 (1.69-1.81) |
| Melanocytic | 45 (11.5) | 429 (19.1) | .003 | 0.60 (0.43-0.83) |
| Pigmentation disorders | 19 (4.9) | 76 (3.4) | .4 | 1.27 (0.75-2.14) |
| Tumors | 35 (9) | 268 (11.9) | .006 | 0.68 (0.40-0.85) |
| Skin appendage involvement | 28 (7.2) | 246 (11) | .4 | 0.83 (0.54-1.27) |
| Exogenous cause | 12 (3.1) | 40 (1.8) | .08 | 1.81 (0.93-3.53) |
Abbreviation: OR, odds ratio
Atopic dermatitis was more frequently observed in foreign children (aOR, 1.65; 95% CI, 1.19-2.31), as was scabies (aOR, 10.6; 95% CI, 4.71-24.10), arthropod bites (aOR, 2.80; 95% CI, 1.14-6.87), and hypopigmentation (aOR, 2.61; 95% CI, 1.06-6.44). In contrast, melanocytic nevus was less frequently observed among foreign children (aOR, 0.50; 95% CI, 0.30-0.83) (Table 3).
Infectious diseases were found more frequently among foreign children (aOR, 1.43; 95% CI, 1.13-1.81), as was erythematous-desquamative disease (aOR, 1.41; 95% CI, 1.69-1.81). Melanocytic processes and neoplastic disease were, however, less common in foreign children (aOR, 0.60; 95% CI, 0.43-0.83 for melanocytic processes; aOR, 0.68; 95% CI, 0.40-0.85 for neoplastic disease) (Table 5).
DiscussionThe present study recorded 3108 visits, of which 14.3% corresponded to foreign children. This proportion is higher than that found in other studies on health care usage for dermatology among adults (approximately 4%),9,11 but is similar to the 13.2% reported by Taberner et al.10
Particularly noteworthy is that the foreign children made more use of walk-in appointments than Spanish children, in agreement with other studies.13,14 A number of explanations are available for the greater reliance on walk-in appointments. For example, foreign parents may be less aware of the normal access pathways or find it harder to attend scheduled appointments due to work constraints. Alternatively, some patients might not have their papers in order. In addition, certain skin diseases in children are a cause of great concern for parents and so a quicker visit is preferred to assuage their anxiety.
An important consideration is where the parents are from. Foreign children in our region originate mainly from Latin America (53.8% of all foreign children), in line with studies performed in the Son Llàtzer hospital in Mallorca, Spain,10 and the Miguel Servet Hospital in Zaragoza,11 (51.7% and 47.1%, respectively). The second most common place of origin was North Africa and Middle East (19.2%), with Eastern Europe in third place (9%). This order is identical to a previous study in our region.15
With regards the frequency of skin diseases and diagnostic categories, in comparison with other pediatric studies that did not take into account origin, our data are similar to those obtained in a pediatric population in Madrid,16 although large differences are apparent compared to those published for the Hospital Universitari Arnau in Vilanova.17 In the latter of these studies, neoplastic disease was reported as frequently as infectious skin disease (mainly because of melanocytic nevus). These 2 types of condition were the most frequent presenting complaint. The authors explain this observation through the high number of referrals for congenital melanocytic nevi by pediatricians and through the possible increase in melanoma in a region where the rates of annual sun exposure are very high.
If we look at the comparison of skin diseases in Spanish and foreign children, we see that foreign children are at almost twice the risk of suffering atopic dermatitis. In studies performed in Europe and Australia, a higher prevalence of atopic eczema was reported in certain immigrant pediatric populations, such as for example in black children18 and Asian children.19
The only infection reported more frequently in foreign children was scabies, with a 10-fold higher risk. Previous studies had suggested that scabies was more frequent in foreign children,20 with greatest prevalence among Asian children in a study in Madrid.21 In a recent study in Greece, scabies was reported twice as often among foreign children, although bacterial infections were also twice as frequent in that study, unlike in our study.8 The fact that this disease and others such as bites are more frequent in foreign children could be related to their socioeconomic status as they probably live in homes with worse hygiene and less effective means for keeping out arthropods and flying insects.
With regards the diagnostic categories, erythematous-desquamative and infectious disease were significantly more frequent in foreign children compared to Spanish ones. These 2 categories, along with the third most frequent category, melanocytic lesions, accounted for 70.5% of all disease, although this latter category was significantly more frequent in Spanish children, as was also the case for neoplastic disease.
Among children whose presenting complaint was a melanocytic lesion, foreign children had a 50% lower risk of having melanocytic nevus. This trend was reversed in the case of congenital nevus, which was approximately twice as common in the foreign population with melanocytic lesions. These data are in agreement with those of Albares et al.15 and with those of Monteagudo et al.22 in a study that analyzed neonatal disease.
This study is subject to a series of limitations. First, as this was a cross-sectional, observational study, patients were not followed up over time and certain skin conditions might therefore not have been detected. In addition, the variables analyzed were collected by different dermatologists and so interobserver variations may be present.
We can conclude that there appear to be differences in the way of seeking medical care for foreign children and Spanish children for skin diseases. We believe that awareness of these differences will help us design more effective dermatologic health promotion programs for these children.
Ethical ResponsibilitiesProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed their hospital's protocol on the publication of data concerning patients and that all patients included in the study have received sufficient information and have given their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that patient data do not appear in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Pérez-Crespo M, Ramos-Rincón JM, Albares-Tendero MP, Betlloch-Mas I. Estudio comparativo epidemiológico de la enfermedad cutánea en población infantil inmigrante y autóctona en Alicante. Actas Dermosifiliogr. 2014;105:394–400.


