


A 7-month-old boy with no past history of interest was referred to the dermatology department for evaluation of a tongue ulcer that had appeared 1 month earlier. The mother stated that the ulcer was painful and that it had appeared at the same time as eruption of the lower incisor teeth. Treatment with topical corticosteroids had produced no improvement.
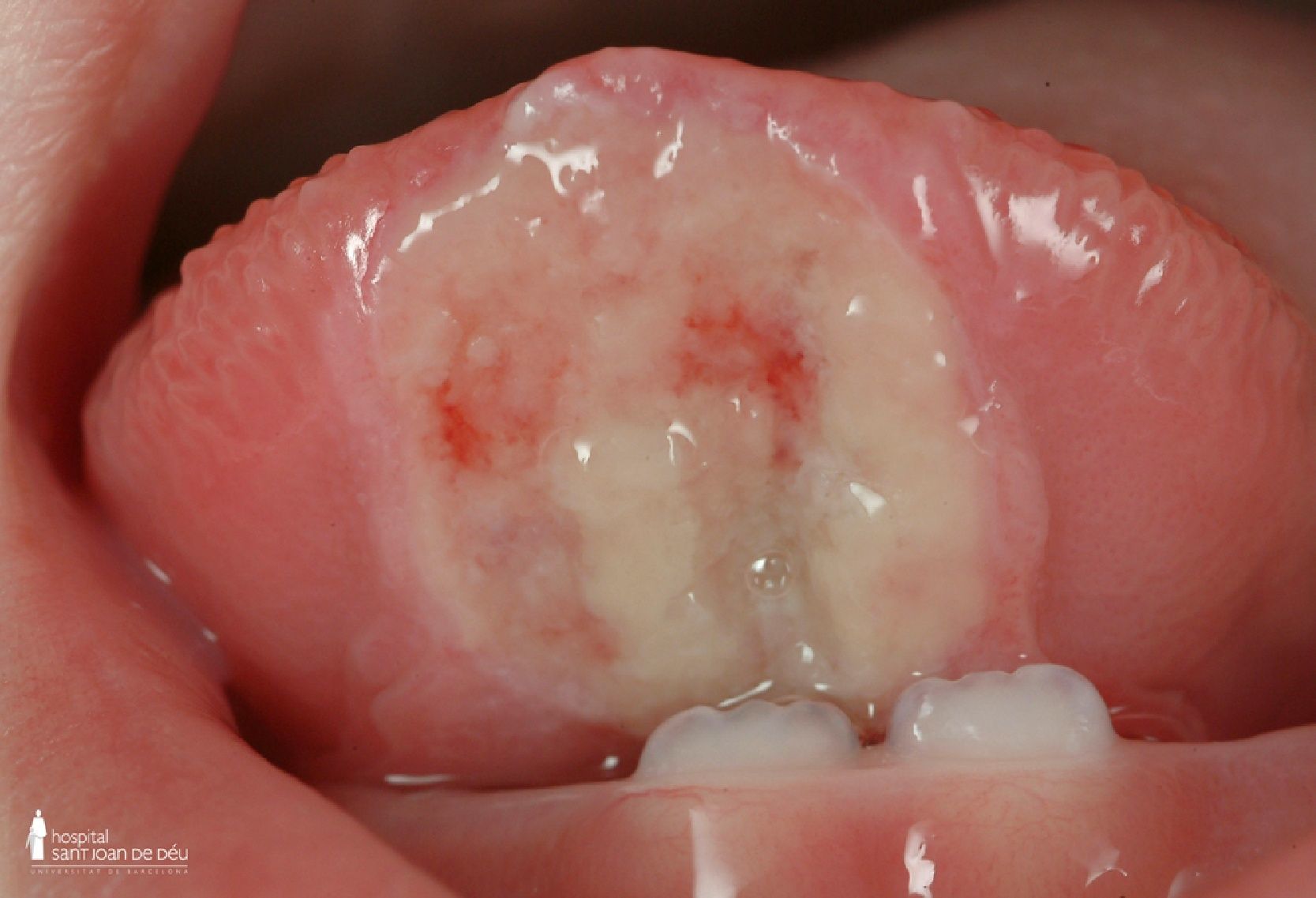
Physical ExaminationOn examination, the infant presented a round indurated ulcer that measured 1×1cm and had well-defined borders. The ulcer was situated on the ventral surface of the tongue, coincident with the lower incisor teeth (Fig. 1). A whitish exudate covered the base of the lesion, in which there were 2 deeper linear ulcers. There were no palpable cervical lymph nodes and no other skin or mucosal lesions. The child presented good height and weight gain and neurological examination was normal.
Additional Tests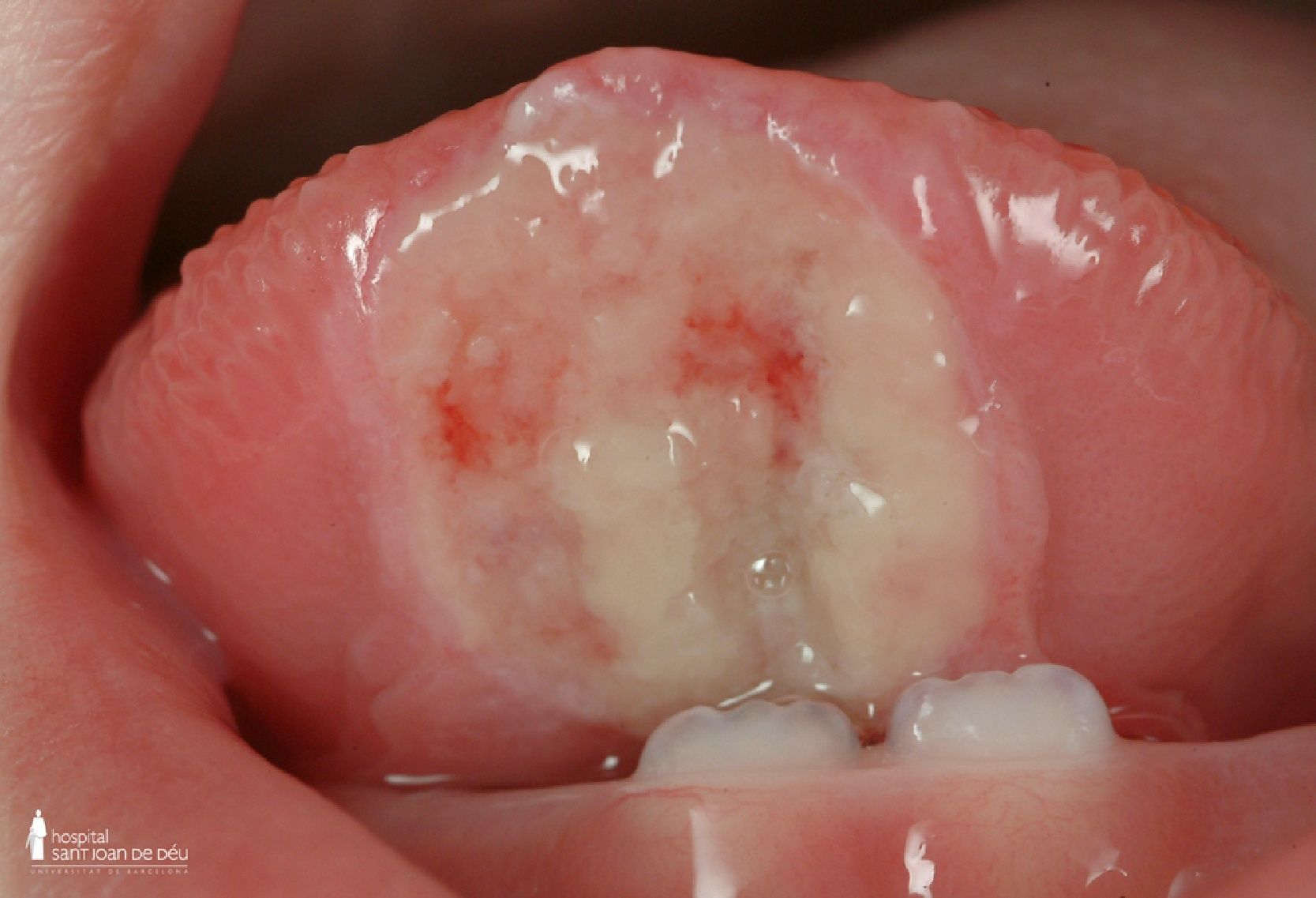
Bacterial culture and polymerase chain reaction analysis for herpes 1 and 2 viruses, Epstein-Barr virus, and cytomegalovirus were negative. Based on the initial clinical suspicion, and given the age of the patient, skin biopsy was not performed.
What Is Your Diagnosis?
DiagnosisRiga-Fede disease.
Clinical Course and TreatmentThe patient received dental treatment with smoothing of the edges of the incisor teeth. At 4 weeks the lesion had reduced in size (Fig. 2), and a month later it had completely disappeared.
Comment
The first clinical description of Riga-Fede disease was made by Antonio Riga in 1881, and its histological features were described by Francesco Fede in 1890.1 It is an uncommon, benign condition characterized by an ulcer on the oral mucosa of children aged less than 2 years.2,3 In adults the disease is known as eosinophilic ulcer of the oral mucosa, traumatic granuloma of the tongue, or eosinophilic granuloma of the tongue, among other names.1
The ulcer is situated on the ventral surface and tip of the tongue in the majority of cases,2,3 and the incidence is similar in both sexes.4 The etiology is believed to be recurrent trauma secondary to continual movements of protrusion and retraction of the tongue over the lower incisor teeth.3,5
Riga-Fede disease is usually observed in children with premature eruption of the teeth, whether natal or neonatal.5,6 It may also be observed in children with neurological diseases or cerebral palsy, and it can even be the initial manifestation of neurological diseases such as familial dysautonomia (Riley-Day syndrome), congenital autonomic dysfunction with universal pain loss, or Lesch-Nyhan syndrome.2–6 Domingues-Cruz et al.6 proposed a classification based on age at onset and associated diseases. Early cases (before 6 months of age) are caused by natal or neonatal teeth, and there is no association with neurological disorders, whereas late cases (after 6 months of age) are caused by the primary dentition and may be associated with neurological or developmental diseases.
Infections (including congenital syphilis, tuberculosis, and candidiasis), tumors (lymphoma, sarcoma, myofibroma, granular cell tumor), and hematological diseases (agranulocytosis) must be considered in the differential diagnosis.2,4,6
Biopsy reveals an ulcer with granulation tissue and a diffuse, mainly eosinophilic infiltrate that extends down to the muscle.1
The most common complications are bleeding and pain, which may interfere with feeding and lead to malnutrition, dehydration, and even delayed development.4
Recommended treatments include planing or smoothing of the incisal edges of the lower incisor teeth or tooth protection with caps or composite increments to the teeth. Extraction of the incisor teeth is indicated as a last resort for persistent ulcers.4,5
Riga-Fede disease should be included in the differential diagnosis of oral ulcers in children. Clinical recognition of this disease will prevent unnecessary biopsy or surgery. Children with Riga-Fede disease should undergo dental examination as well as neurological evaluation to exclude neurological disease.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: del Alcázar–Viladomiu E, et al. Úlcera lingual en un lactante de 7 meses. Actas Dermosifiliogr. 2013;104:631–2.



