


Hand hygiene is the most important measure for the prevention of nosocomial infection. We describe the different products available for hygiene and antisepsis of the hands and the use of these products in daily practice. Hand hygiene products such as soaps and detergents are a cause of irritant dermatitis in health professionals. This irritation is one of the principal factors affecting their use in clinical practice. Alcohol-based products are better tolerated and less irritant than soap and water; irritation should not therefore be a limiting factor in the use of these products and they are to be recommended in place of soap and water. Informative and continued education programs could increase their use.
La higiene de manos es la medida más importante para la prevención de la infección nosocomial. Describimos los diferentes productos para la higiene y antisepsia de las manos y su modo de empleo en la práctica clínica habitual,. Los productos de higiene de manos, sobre todo jabones y detergentes, son causa de dermatitis irritativa en los profesionales sanitarios. Esta irritación cutánea que producen es uno de los principales motivos que condicionan su empleo en condiciones reales. Los productos de base alcohólica presentan mejor tolerancia dérmica y son menos irritantes que el lavado con agua y jabón, por lo que la irritación no debe ser un factor limitante para la utilización de éstos, que deben recomendarse en mayor medida que el lavado con agua y jabón. Los programas educacionales de información y formación continuada podrían aumentar su utilización.
The hands of health care personnel act as vectors in the transmission of microorganisms and are one of the main mechanisms of transmission of nosocomial infection.1–3 Hand hygiene is the most important measure for the prevention of nosocomial infection and one of the cornerstones of programs for the control and prevention of infections in hospitals. Proper hand hygiene can reduce the transmission of infection by up to 40%.1,3–7 However, compliance with antisepsis protocols among health professionals needs to be improved. Diverse reasons are cited for this lack of compliance, including lack of time and lack of familiarity with the recommendations, but skin irritation caused by hygiene products is one of the reasons why personnel perform hand hygiene on less than half of the occasions when it is indicated.2–4,6
We describe the different products available for hand hygiene, their use in everyday clinical practice, and their relationship with hand eczema in health care personnel.
Products Available for Hand Hygiene and Antisepsis, and Methods of UseHand Hygiene ProductsThe most widely used hand hygiene products can be classified into the following 3 categories:
- a)
Hydroalcoholic liquid rubs. These rubs contain alcohol (most often ethanol, n-propanol, and isopropanol), which acts as an antiseptic. They also contain surfactants, which add a wetting, emulsifying, and foaming action, and emollients or other skin conditioning agents to prevent the skin from drying.4,8,9
- b)
Alcohol-based gel rubs. Another type of hand sanitizing product is the alcohol-based antiseptic in a gel formulation. These products are very similar in composition to the liquid rubs and have an alcohol content of between 60% and 75%. The alcohol most often used is ethanol, but some of these products combine ethanol with 1-propanol or 2-propanol. The consistency of these gels is achieved by way of a thickening system that increases their viscosity. This thickening system does not penetrate the skin and after continuous application the hands are coated in a moist layer of the amine salts of polyacrylic acid.10
- c)
Antiseptic soaps. The active ingredients in antiseptic soaps are usually chlorhexidine and triclosan.1 Other components used are chloroxylenol, hexachlorophene, iodides such as povidone-iodine, and quaternary ammonium compounds.11
The antimicrobial efficacy of each type of hand hygiene product is different.
- a)
Hydroalcoholic liquid rubs. Alcohols, such as ethanol, 1-propanol, and 2-propanol have a broad spectrum of antimicrobial activity. They are bactericidal, virucidal, fungicidal, and mycobactericidal, but have virtually no sporicidal activity. In addition, the alcohols are fast-acting (20–30seconds) and they reduce the colonization of the skin more effectively than washing with soap and water.1,3,4,6,8,9,12,13 Hydroalcoholic solutions are also suitable for surgical antisepsis. They immediately achieve a level of efficacy similar to that of soaps and detergents, but the effect is more long-lasting.5,9,14 The guidelines of the World Health Organization Center for Disease Control and Prevention clearly recommend the use of water-alcohol solutions for hygienic hand antisepsis.8,11,13,15
- b)
Alcohol-based gel rubs. The literature reviewed indicated that most of the alcohol-based gel rubs on the market have significantly less antibacterial activity than hydroalcoholic solutions.1,5 However, there are currently some alcohol-based gel products marketed for hand hygiene in a 30-second application that do meet European Standard EN 1500. Alcohol-based gels with the same spectrum of antimicrobial activity as hydroalcoholic liquid rubs are suitable and effective for use in hospitals.1,16
- c)
Antiseptic soaps. The antimicrobial spectrum of chlorhexidine and triclosan is narrower than that of the hydroalcoholic solutions and their microbial activity is slower.1 A number of comparative studies have shown chlorhexidine to be a better antiseptic than povidone-iodine because of its faster action and greater residual antimicrobial activity.17
For the purposes of this article we will use the term alcohol-based products to refer to both liquid and gel alcohol-based rubs, but with the stipulation that the alcohol-based gels used must have at least the same antimicrobial efficacy as the hydroalcoholic solutions.
Hand Hygiene in Everyday Clinical PracticeThere are 3 types of hand hygiene procedures1,4,15:
- a)
Social or hygienic washing with plain soap and water. This type of handwashing does not eliminate certain microorganisms, even after several washes.
- b)
Washing with water and antiseptic soap. Handwashing with antiseptic soap removes dirt, organic matter, transient flora, and some of the resident flora; it also has some residual antimicrobial activity.
- c)
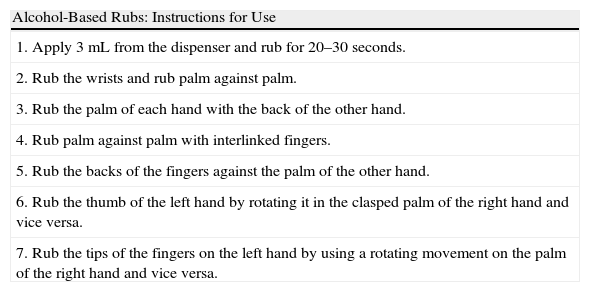
Antisepsis with alcohol-based hand rubs. Prior to use, there should be no visible dirt on the hands and after application the hands must be rubbed together until the alcohol has evaporated and they are completely dry. All personnel must learn the appropriate application technique, which involves coating the entire surface of the hands to ensure efficacy. The correct procedure is described in Table 1.4
Table 1.Instructions for Using Alcohol-Based Rubs.
Alcohol-Based Rubs: Instructions for Use 1. Apply 3mL from the dispenser and rub for 20–30seconds. 2. Rub the wrists and rub palm against palm. 3. Rub the palm of each hand with the back of the other hand. 4. Rub palm against palm with interlinked fingers. 5. Rub the backs of the fingers against the palm of the other hand. 6. Rub the thumb of the left hand by rotating it in the clasped palm of the right hand and vice versa. 7. Rub the tips of the fingers on the left hand by using a rotating movement on the palm of the right hand and vice versa.
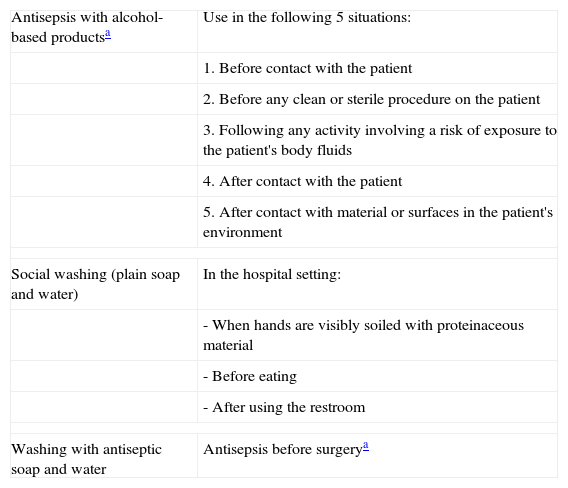
The indications for the different hand hygiene procedures are shown in Table 2.1,2,4,10,15,18,19
Indications for Different Hand Hygiene Procedures.
| Antisepsis with alcohol-based productsa | Use in the following 5 situations: |
| 1. Before contact with the patient | |
| 2. Before any clean or sterile procedure on the patient | |
| 3. Following any activity involving a risk of exposure to the patient's body fluids | |
| 4. After contact with the patient | |
| 5. After contact with material or surfaces in the patient's environment | |
| Social washing (plain soap and water) | In the hospital setting: |
| - When hands are visibly soiled with proteinaceous material | |
| - Before eating | |
| - After using the restroom | |
| Washing with antiseptic soap and water | Antisepsis before surgerya |
Source: Adapted from Kampf1, Cabrillana Molina et al.2, Delgado-Gil et al.4, Pietsch10, Boyce et al.15, Pedersen et al.18 and Kampf et al.19
Alcohol-based products can also be used for surgical antisepsis5,9,14 (the term alcohol-based products includes hydroalcoholic solutions and alcohol-based gels, provided that the latter have at least the same antimicrobial activity as the solutions).
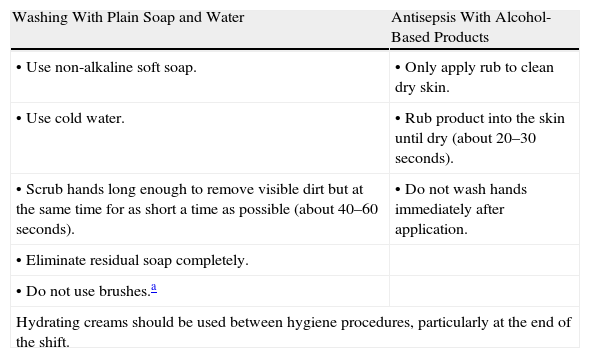
Table 3 shows instructions for the use of the different types of hand hygiene products.1,11,13,19
Recommendations for Hand Hygiene in Hospitals.
| Washing With Plain Soap and Water | Antisepsis With Alcohol-Based Products |
| • Use non-alkaline soft soap. | • Only apply rub to clean dry skin. |
| • Use cold water. | • Rub product into the skin until dry (about 20–30seconds). |
| • Scrub hands long enough to remove visible dirt but at the same time for as short a time as possible (about 40–60seconds). | • Do not wash hands immediately after application. |
| • Eliminate residual soap completely. | |
| • Do not use brushes.a | |
| Hydrating creams should be used between hygiene procedures, particularly at the end of the shift. | |
Other important aspects that must be taken into consideration with respect to hand hygiene are outlined below.
- 1.
Hot water should not be used to wash hands.4,19
- 2.
As indicated above, hands should not be dried following the application of alcohol-based products (the alcohol should be allowed to evaporate).4
- 3.
The use of alcohol-based products excludes hand washing and hands should not be washed before or after applying such products.4,11,13
- 4.
Handwashing before antisepsis predisposes the skin to toxic reactions and removes the natural sebum layer that protects the skin, thereby increasing skin irritation and dryness; handwashing may also decrease bactericidal efficacy.13,20
- 5.
Handwashing with soap and water after hygienic hand disinfection will, in addition to removing the superficial sebum layer, also remove the emollients that are included in the alcohol-based product, thereby increasing the risk of dermatitis.4,13
- 6.
Alcohol-based products should not be used on wounds as they may damage the tissue.4
- 7.
Hands should be washed before eating and after using the restroom. Sanitization with alcohol-based products in these circumstances is not suffiicient.4
- 8.
The use of gloves does not obviate the need for hand hygiene and is not a substitute for antisepsis; in fact, gloves should only be worn when necessary. Hands should always be dry before gloves are put on as damp hands increase irritation and the rate of glove perforation.19
- 9.
In view of the possibility of microbial colonization and cross-transmission of nosocomial infections, the following points should not be forgotten: rings and bracelets are easily colonized; gloves must be worn when touching mucous membranes or nonintact skin; the same pair of gloves should never be used with a different patient or with the same patient when moving from a contaminated to a clean site.4
Frequent and repeated use of hand hygiene products, particularly soaps and other detergents, is the leading cause of irritant contact dermatitis among health workers. These products can damage the skin through denaturation of stratum corneum proteins, changes in intercellular lipids, as well as decreased corneocyte cohesion and stratum corneum water-binding.11 As a result, they provoke changes in the skin flora of the hands and favor transient colonization. Damage can be exacerbated by the use of hot water, failure to apply hand cream, and drying hands with poor quality paper towels.4,11
Alcohols have practically no irritant effect and are considered to be among the safest antiseptics.20,21 There is no difference in the dermal tolerance of these products between atopic and nonatopic patients and, even in pre-irritated skin, the damage caused by alcohols is very low.13,14,21 The low irritancy potential and better skin tolerance of commonly used alcohols as compared to soaps and detergents have been demonstrated by patch tests and bioengineering methods such as the measurement of transepidermal water loss (a measure of skin barrier disruption) and corneometry, which measures skin hydration.6,8,11–14,21,22 The authors of various studies have reported no increase in skin barrier disruption or erythema after patch tests with 1-propanol, 2-propanol, and ethanol; however, a slight decrease in corneometric values was observed, indicating a decrease in skin hydration.20,21 The drying effect of alcohol can be reduced or eliminated by the use of emollients such as glycerin. Alcohol-based sanitizers must contain emollients and they consequently have moisturizing properties despite their high alcohol content.5,22
The risk of sensitization to alcohol is low even in high-risk groups such as health care personnel.12,14,21 Contact allergy to alcohol is very rare, and only sporadic cases of type IV hypersensitivity to ethanol, 1-propanol, and 2-propanol have been reported.11,12 Isolated cases of contact urticaria and anaphylactoid reactions have also been reported. However, commercially available alcohol-based products are rarely pure, and it is the impurities and contaminants that are responsible for most reactions to such products.11
Why Do Most Health Professionals Believe That Alcohol-Based Products Are Strong Irritants That Cause Dermatitis?Even though the use of alcohol-based rubs has been promoted as an effective antiseptic procedure offering excellent dermal tolerance and the possibility of increasing the frequency of performing correct hand hygiene, acceptance of these products has been poor.12 One reason for this is that products containing alcohol produce a burning sensation when applied to pre-irritated skin. The alcohol easily penetrates the skin through the disrupted barrier and stimulates receptors that cause a burning sensation even though the product does not increase irritation or damage the skin. Increasingly, this effect has led health care workers to wash their hands rather than use alcohol-based rubs despite the minimal irritancy potential of these products. However, while handwashing does not cause discomfort or give rise to an immediate sensation of irritation, it further disrupts the skin barrier function and perpetuates the vicious circle that often leads to irritant dermatitis.12–14,19–21 The presence of irritation is interpreted by some users as an allergy, which leads them to consult a specialist and undergo patch testing with negative results.12,13,19,21
The burning sensation experienced when alcohol-based products are applied should be interpreted as a sign of changes in skin barrier function and a predictor of hand dermatitis.13,19–21
The Importance of Using Alcohol-Based Products to Prevent Hand Eczema Among Health ProfessionalsThe dermatologist should be aware that alcohol-based products are not the leading cause of dermatitis among health professionals, but rather an important factor in the prevention and treatment of this condition. Alcohol rubs are an essential tool for the control of nosocomial infections and dermatologists should not contribute to the misconceptions that reduce their correct and frequent use.
Medical personnel who report discomfort when they apply alcohol-based products should be prescribed treatment for irritant dermatitis (which is usually subclinical) and advised to continue using alcohol-based products whenever these are indicated.
Several studies have shown that it is not enough to simply introduce alcohol-based products into the workplace to reduce the prevalence of occupational dermatitis and increase compliance with recommended hand hygiene procedures: educational programs explaining the mechanisms of irritation and irritants and the advantages of alcohol-based rubs over handwashing are also important.2,3,6,11–13,19,23–25
Other important measures shown to increase compliance with the use of alcohol-based sanitizing rubs are ensuring the availability of and ease of access to these products,19 and avoiding their introduction during winter months. When temperatures are low and the weather is more humid, hands are more likely to become dry, and users may attribute these changes to the new products rather than to climatic factors.12
Summarizing the information in this paper, we propose an algorithm for the selection of hand hygiene products and the management of the skin conditions associated with the use of such products (Fig. 1).

Indications for the use of hand hygiene products and an algorithm for the therapeutic management of contact dermatitis. The figure shows a dynamic model of how the dermatitis will progress to a more severe condition if not properly treated. ICD indicates irritant contact dermatitis.
Hand hygiene products are essential for the control of nosocomial infection. However, these products—particularly soaps and detergents—are the leading cause of irritant contact dermatitis in health care personnel.11,17,20,23 We recommend the use of alcohol-based products as standard procedure for hand hygiene because their low irritancy potential and superiority to other products in terms of dermal tolerance have been demonstrated; they also more effectively reduce the bacterial load.4,6,8,11,13,15,25 Despite the widespread availability of alcohol-based products in the workplace, compliance remains low.5 As dermatologists, we can play an important role by using and providing a model for the use of these sanitizing rubs in our work. It is important that we correctly inform and advise the medical personnel who consult us for irritant contact dermatitis and stress the low irritancy potential of alcohol-based products.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
We would like to thank Dr. Francisco Vázquez Vizoso for his critical reading of this manuscript.
Please cite this article as: Batalla A, et al. Productos de hygiene y antisepsia de manos: su empleo y relación con el eccema de manos en los profesionales sanitarios. Actas Dermosifiliogr. 2012;103:192–7.



