

Some types of cancer tend to spread to certain organs. In the case of melanoma, uveal melanoma spreads almost exclusively to the liver, while cutaneous melanoma spreads to the liver and other organs. Although important advances have been made in our understanding of the molecular mechanisms underlying melanoma, few recent studies have focused on the patterns of visceral metastasis in cutaneous melanoma. The aim of this study was to retrospectively investigate whether clinicopathologic variants of cutaneous melanoma and primary tumor site might be associated with pattern and time of onset of metastasis to visceral sites, including the central nervous system (CNS).
Materials and methodsWe included patients diagnosed with cutaneous melanoma between 1988 and 2009 with at least 2 years’ follow-up.
ResultsOf the 1083 patients studied, 92 developed visceral metastasis. The CNS was affected in 21 cases, the lungs in 24, the liver in 17, the digestive tract in 7, and multiple organs simultaneously in 23. Metastasis to the lungs, the liver, and the digestive tract occurred within 5 years in most cases, while metastasis to the CNS and multiple organs occurred later (>5 years in 38% and 43% of cases, respectively).
ConclusionsUnlike uveal melanoma, cutaneous melanoma spreads to different organs without any particular predilection. We observed no significant associations between the site of visceral metastasis and either clinicopathologic variant or location of the primary tumor. Metastasis occurred within 5 years of diagnosis in most cases, but it can occur after 10 years.
Algunas formas de cáncer tienden a producir metástasis en determinados órganos. En cuanto al melanoma, el melanoma uveal produce metástasis casi exclusivamente en el hígado, mientras que el melanoma cutáneo se disemina también a otros órganos. A pesar de importantes avances en el conocimiento de las bases moleculares del melanoma, hay pocos estudios recientes sobre el patrón de diseminación visceral del melanoma cutáneo. Nuestro objetivo fue analizar retrospectivamente una posible asociación entre tipo clinicopatológico y localización del melanoma cutáneo con el patrón de diseminación visceral y su cronología.
Material y métodosSe incluyeron en el estudio los pacientes diagnosticados de melanoma cutáneo entre 1988–2009 con más de 2 años de seguimiento.
ResultadosDe un total de 1.083 pacientes 92 desarrollaron metástasis viscerales: 21 en el sistema nervioso central (SNC), 24 en los pulmones, 17 en el hígado, 7 en el tubo digestivo y 23 en múltiples órganos simultáneamente. Las recidivas en el pulmón, el hígado y el tubo digestivo se produjeron mayoritariamente antes de los 5 años, mientras que las metástasis al SNC y a múltiples órganos simultáneamente fueron más tardías (38 y 43% después de los 5 años respectivamente).
ConclusionesA diferencia del melanoma ocular, el melanoma cutáneo se disemina por igual a múltiples órganos. No hemos detectado asociación significativa respecto al órgano diana de las metástasis según el tipo histológico y tampoco según la localización del tumor primario. A pesar de que la mayoría de metástasis viscerales se producen antes de los 5 años, también pueden producirse metástasis viscerales más allá de los 10 años de seguimiento.
Some forms of cancer are known to metastasize to certain organs or tissue. Visceral metastases from cutaneous melanoma are usually located in the lung, central nervous system (CNS), liver, or bone,1 whereas uveal melanoma spreads almost exclusively to the liver.2,3 Although there have been substantial advances in our knowledge of the molecular mechanisms underlying the different types of melanoma,4–6 there have been few recent studies of the pattern of visceral dissemination of cutaneous melanoma.
The aim of this retrospective study was to investigate whether clinicopathologic type and melanoma site are associated with the pattern and timing of visceral dissemination.
Material and MethodsThe study included all patients with cutaneous melanoma diagnosed in the Hospital de Bellvitge, Barcelona, Spain, between 1988 and 2009. This university hospital provides tertiary care to approximately 1 million people.
In situ melanomas were excised with a 5-mm margin and the margins for invasive melanomas were determined by the maximum depth of invasion (Breslow thickness): melanomas of less than 1mm were excised with 1-cm margins, those with a depth of between 1.01 and 2mm with 2-cm margins, and those with a depth of more than 2mm with 3-cm margins. Before 2000, regional lymph nodes were removed when the Breslow thickness was greater than 1.5mm if the melanoma was located on the limbs. When the melanoma was located on the trunk or head, lymph node dissection was only performed when the primary tumor lay adjacent to a lymphatic basin considered likely to receive drainage from the primary tumor. After 2000, sentinel lymph node biopsy was performed for all melanomas with a Breslow thickness greater than 1mm, with regional lymph node removal in the event of sentinel lymph node involvement.
For the first 2 years after diagnosis, patients returned to the dermatology department every 4 months for clinical follow-up. Subsequently, visits were every 6 months for the next 5 years. Patients with a Breslow thickness of less than 1mm were followed for 5 years and then referred to their local dermatologist for annual check-ups for the rest of their lives. Patients with a Breslow thickness of more than 1mm were followed for at least 10 years in the dermatology department and then referred to their local dermatologist for annual check-ups for the rest of their lives. During the first 2 years of follow-up, laboratory tests including measurement of lactate dehydrogenase were performed at each visit. A chest radiograph was taken annually, and other tests were ordered according to the clinical and laboratory findings.
Clinical data were extracted retrospectively from the medical records of the patients and entered into a database to which only the authors of this present article had access. The clinical data collected included sex, age at time of diagnosis, date of diagnosis, primary tumor site, date of visceral metastasis, and pattern of visceral metastasis. The patterns of visceral dissemination were defined according to the first organ to which the melanoma spread. The organs were classified as CNS, lung, liver, digestive tract, and multiple organs (when the tumor spread simultaneously to more than 1 organ). The histological data reviewed were the clinicopathologic type of melanoma, the maximum depth of invasion or Breslow thickness, Clark level, and presence of ulceration.
For the statistical analysis, quantitative variables were compared by analysis of variance and qualitative variables by contingency tables. The χ2 test was often not applicable given the low number of cases, and we could only estimate the presence of correlations. The statistical package used was SPSS 13.0 for Windows. A P value less than .05 was considered statistically significant.
ResultsA total of 1083 patients with cutaneous melanoma diagnosed between 1988 and 2009 had completed at least 2 years of follow-up in the dermatology department of the Hospital de Bellvitge (435 men and 648 women with a mean [SD] age of 53.72 [17.50] years). Of these, 92 patients had developed visceral metastases during this period (50 men and 42 women aged between 26 and 86 years and with a mean [SD] age of 55.41 [16.17] years). The first visceral metastasis was to the CNS in 21 cases, to the lung in 24 cases, to the liver in 17 cases, and to the digestive tract in 7 cases. Simultaneous spread to multiple organs occurred in 23 patients. Table 1 shows the distribution of the pattern of visceral metastasis by sex, clinicopathologic type of melanoma, and primary tumor site.
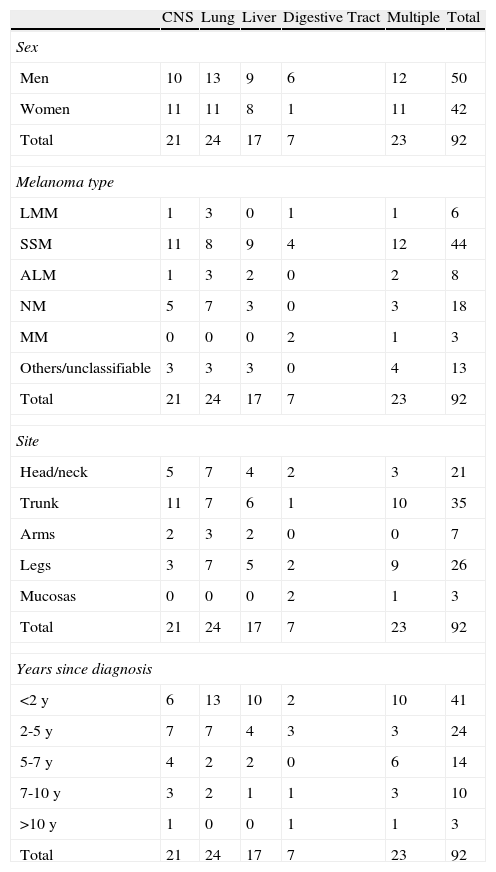
Pattern of Visceral Metastasis According to Sex, Clinicopathologic Type of Melanoma, Primary Tumor Site, and Time From Diagnosis of Melanoma to Development of First Visceral Metastasis.
| CNS | Lung | Liver | Digestive Tract | Multiple | Total | |
| Sex | ||||||
| Men | 10 | 13 | 9 | 6 | 12 | 50 |
| Women | 11 | 11 | 8 | 1 | 11 | 42 |
| Total | 21 | 24 | 17 | 7 | 23 | 92 |
| Melanoma type | ||||||
| LMM | 1 | 3 | 0 | 1 | 1 | 6 |
| SSM | 11 | 8 | 9 | 4 | 12 | 44 |
| ALM | 1 | 3 | 2 | 0 | 2 | 8 |
| NM | 5 | 7 | 3 | 0 | 3 | 18 |
| MM | 0 | 0 | 0 | 2 | 1 | 3 |
| Others/unclassifiable | 3 | 3 | 3 | 0 | 4 | 13 |
| Total | 21 | 24 | 17 | 7 | 23 | 92 |
| Site | ||||||
| Head/neck | 5 | 7 | 4 | 2 | 3 | 21 |
| Trunk | 11 | 7 | 6 | 1 | 10 | 35 |
| Arms | 2 | 3 | 2 | 0 | 0 | 7 |
| Legs | 3 | 7 | 5 | 2 | 9 | 26 |
| Mucosas | 0 | 0 | 0 | 2 | 1 | 3 |
| Total | 21 | 24 | 17 | 7 | 23 | 92 |
| Years since diagnosis | ||||||
| <2 y | 6 | 13 | 10 | 2 | 10 | 41 |
| 2-5 y | 7 | 7 | 4 | 3 | 3 | 24 |
| 5-7 y | 4 | 2 | 2 | 0 | 6 | 14 |
| 7-10 y | 3 | 2 | 1 | 1 | 3 | 10 |
| >10 y | 1 | 0 | 0 | 1 | 1 | 3 |
| Total | 21 | 24 | 17 | 7 | 23 | 92 |
Abbreviations: ALM, acral lentiginous melanoma; CNS, central nervous system; LMM, lentigo maligna melanoma; MM, mucosal melanoma; NM, nodular melanoma; SSM, superficial spreading melanoma.
We did not observe any significant differences between sexes with respect to target organ of the visceral metastases. Analysis by clinicopathologic type of melanoma revealed that the lung was the most common target organ for lentigo maligna melanoma, acral lentiginous melanoma, and nodular melanoma (although the differences were not statistically significant) and that superficial-spreading melanoma showed no preference for any organ. We detected no significant association between the pattern of visceral spread and the different primary tumor sites.
The mean (SD) age of the 92 patients with visceral metastases was 55.41 (16.17) years and the Breslow thickness of the tumors ranged from 0.35 to 14mm, with a mean (SD) of 3.98 (3.17)mm. There were no significant differences in age of the patient or Breslow thickness of the primary tumor according to metastatic site in the analysis of variance.
The time between diagnosis of the primary tumor and diagnosis of the visceral metastases ranged from 1 to 148 months (mean [SD] of 38.40 [34.51] months). In 48.2% of patients, this interval was less than 2 years. Table 1 shows the interval between diagnosis and development of the visceral metastases for each pattern of metastatic dissemination. Metastasis to the lung, liver, and digestive tract occurred within 5 years in most patients, whereas metastasis to the CNS occurred later, with 38% of patients having such metastases after more than 5 years of follow-up. Simultaneous metastases to multiple organs occurred later still, with 43% of patients having such metastases after 5 years of follow-up. In 3 cases, visceral metastases occurred after 10 years of follow-up. By means of analysis of variance, significant differences were detected in the mean time to metastasis for different visceral sites (P=.042).
DiscussionMetastatic spread of tumors does not follow a random pattern and different types of cancer may have a predilection for certain organs.7 Expression of chemokines is one of the factors implicated in the preferential spread of a tumor to certain organs.7 Chemokines are responsible for the affinity of leukocytes to lymphoid organs (homeostatic chemokines) and promote extravasation of leukocytes to lesioned or infected tissues during the inflammatory process (inflammatory chemokines). In addition, certain chemokines are specifically expressed in certain organs, where they promote adhesion and migration of tumor cells expressing the corresponding receptors.7 The first study to establish a firm connection between chemokines and organ-specific metastasis showed that the chemokine CXCL12 and its receptor CXCR4 expressed by the tumor cells determined the pattern of dissemination of breast cancer.7 In the case of cutaneous melanoma, certain chemokines have been shown to be implicated in spread to specific target organs.8 Melanomas that express CCR7 and CXR3 tend to spread to lymph nodes9 and those that express CCR9 to the small intestine.10 CCR10 is implicated in cutaneous metastasis11,12 and CCR4 has recently been implicated in the development of brain metastases.12,13
In the case of uveal melanoma, metastasis is usually to the liver.2 One possible mechanism is interaction between hepatocyte growth factor and insulin-like growth factor 1 produced in the liver and its receptors expressed by uveal melanoma cells.3 Recently, an association has been observed between the chemokines CXCR4 and CCR7 and the development of liver metastasis in uveal melanoma.14,15 Uveal melanoma has mutations in the GNAQ gene in 83% of cases,2,3 suggesting that such mutations could specifically favor the mechanisms responsible for liver metastasis. In cutaneous melanoma, 49% of superficial spreading melanomas have BRAF-activating mutations,4,5 27% of nodular melanomas have NRAS mutations,5 and 39% of acral lentiginous melanomas have c-KIT mutations or amplifications.6 These mutations are responsible for cell proliferation in cutaneous melanoma and could in some way be related to a certain expression pattern of chemokines and development of organ-specific metastasis. However, we did not detect any significant association between clinicopathologic type of cutaneous melanoma or primary tumor site and preferential spread to certain organs. These results may indicate indirectly that there is no significant relationship between the mutation responsible for cell proliferation in cutaneous melanoma and the development of organ-specific metastasis.
With regards the timing of development of visceral metastases, metastasis to certain organs such as the lung, liver, and digestive tract appeared early (mostly within 5 years of follow-up), while others, such as metastasis to the CNS and simultaneous metastases to multiple organs, occurred later. Since the guidelines for follow-up of cutaneous melanoma do not include routine imaging follow-up after 5 years,16,17 late visceral metastases are usually detected only when clinical symptoms become apparent and the disease is already very advanced. Simultaneous metastases to multiple organs were the latest to develop in our study (mean time, 51.52 months). It might be supposed that in such cases the tumor cells acquire a late indiscriminate capacity for aggressive invasion and proliferation. However, it is not unusual in cutaneous melanoma for metastases to a single organ to be reported months or years before sudden dissemination to multiple organs, indicating that in such cases melanoma cells are only able to survive in certain organs and that blockade of the mechanisms responsible for selective proliferation to the first target organ could extend patient survival. In animal models, inhibition of the CXCR4/CXCL12 interaction reduced lung metastases.18 Patients with melanomas likely to develop resistance to BRAF/RAS or cKIT inhibitors could also benefit from inhibition of organ-specific metastasis.
The limitations of our study are that it was retrospective and, given the low number of patients, the χ2 test was not applicable in many cases and we could only estimate the presence of correlations.
Unlike uveal melanoma, cutaneous melanoma spreads to different organs without any particular predilection. Although the clinicopathologic type of cutaneous melanoma correlates with certain mutations in the tumor genotype, we did not detect a significant association between the site of visceral metastasis and the clinicopathologic type of cutaneous melanoma. Although most visceral metastases occur within 5 years, we should not forget that visceral spread can develop after more than 10 years of follow-up. Although the yield of follow-up imaging studies is too low to recommend their routine use after 5 years, patients should nevertheless remain in contact with their dermatologist up to 10 years and beyond due to the possibility of late metastases.
Ethical ResponsibilitiesProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all patients included in the study have received sufficient information and have given their informed consent in writing to participate in the study.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Marcoval J, et al. Patterns of Visceral Metastasis in Cutaneous Melanoma: A Descriptive Study. Actas Dermosifiliogr. 2013;104:593–7.



