







Injection of botulinum toxin is currently the most common cosmetic procedure in the United States, and in recent years it has become—together with dermal fillers—the mainstay of therapy for the prevention and treatment of facial aging. However, in some cases the treatment may lead to a somewhat unnatural appearance, usually caused by loss of facial expression or other telltale signs. In the present article, we review the 10 mistakes that should be avoided when injecting botulinum toxin. We also reflect on how treatment with botulinum toxin influences us through our facial expressions, both in terms of how we feel and what others perceive.
La toxina botulínica es la técnica estética más realizada en Estados Unidos, y en los últimos años se ha convertido, junto con los rellenos, en el eje de la prevención y el tratamiento del envejecimiento facial. Sin embargo, hay ocasiones en que se obtienen resultados poco naturales, bien debido a una inhibición marcada de la expresión, bien por determinados signos que «delatan» que una persona ha sido infiltrada. En este artículo revisamos los 10 errores que han de evitarse cuando se infiltra toxina botulínica. Adicionalmente, reflexionamos sobre la influencia de la toxina botulínica a través de nuestra gesticulación, tanto en lo que sentimos como en lo que sienten los demás.
According to the American Society of Plastic Surgeons, injection of botulinum toxin is currently the most common cosmetic procedure in the United States. The use of botulinum toxin to eliminate expression lines by relaxing the facial muscles has become—together with dermal fillers—the mainstay of therapy for the prevention and treatment of facial aging.1
Patients considering injectable treatments generally want natural-looking, minimally detectable results. However, a nonnegligible portion of the population believes that the use of botulinum toxin—or Botox, as it is commonly known—produces unnatural and, in many cases, grotesque results.
In our opinion, there are 2 general reasons why some people hold this opinion:
- -
In some cases, the results of the technique can be too “paralyzing,” leading to a loss of facial expressiveness.
- -
In other cases, an unnatural eyebrow shape and new telltale wrinkles signal that a patient has received botulinum toxin injections.
However, when used prudently and rigorously by a doctor who understands the anatomy and functionality of the facial muscles, botulinum toxin injection is clearly, for both doctor and patient, the most gratifying technique used in the fascinating field of cosmetic dermatology. Moreover, in our experience, botulinum toxin has an “educating” effect on the facial muscles and therefore also helps to prevent the appearance of certain expression lines.
Proper technique is essential to achieving good results with botulinum toxin. In this article, we analyze the mistakes that doctors should avoid in order to achieve optimal results with botulinum toxin injection.
Five Errors of ActionUsing an Excessively High DoseResult: Lack of ExpressionSome articles and textbooks recommend using a dose of 20-40 U of botulinum toxin type A (Vistabel) in the glabella, 15-30 U in the forehead, and 12-30 U in the crow's feet.2,3 We use 30% less in the glabella, 50% less in the forehead, and the same dose in the crow's feet. On the lower third of the face, we usually use 50% less than the generally recommended dose. With this approach, the results are more natural and side effects are less frequent; however, patients should be informed that the effect of the procedure will last for a shorter time (approximately 3-4 months).
In our protocol, we ask patients to return for a follow-up appointment 2 weeks after the initial treatment. At this visit, we reassess the patient and, if necessary, administer additional injections in certain areas. However, it is important to educate patients to help them understand that “less is more” (ie, the goal is not to completely paralyze the facial muscles).
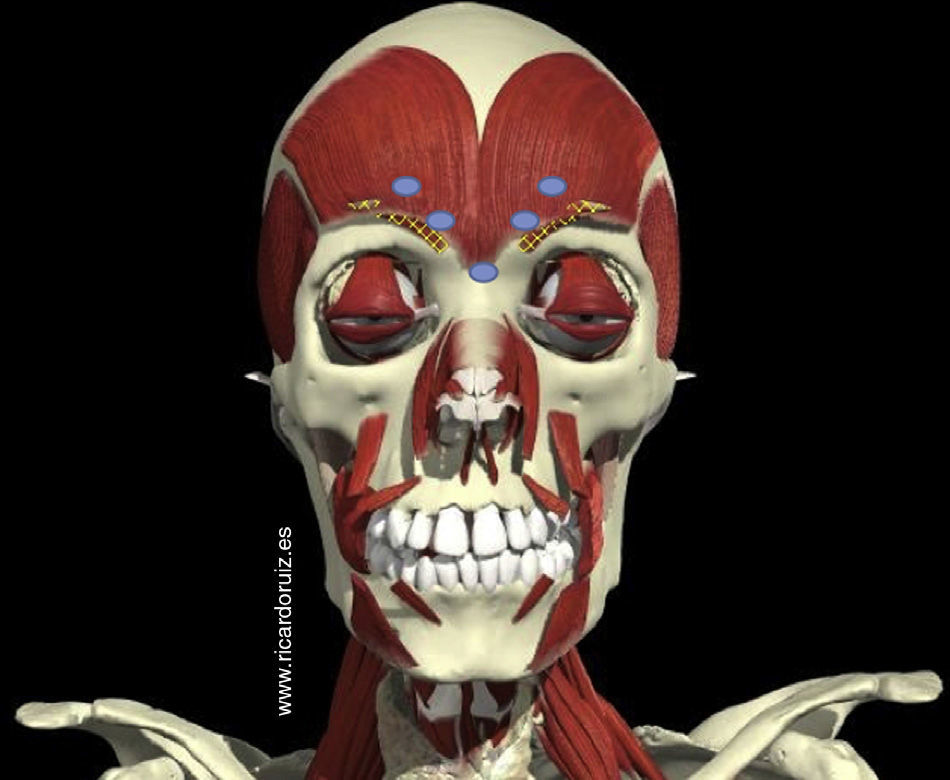
Injecting the Frontalis Muscle Instead of the Corrugator Supercilii MuscleResult: Mephisto EffectThe 5 traditional glabellar injection sites appear in many articles and textbooks (Fig. 1). In reality, however, the 2 most superior of these injection sites are not located on the corrugator supercilii muscle—for which the insertion site is almost at eyebrow level—but rather on the frontalis muscle. Relaxation of the frontalis muscle causes the medial portion of the brow to descend and lifts the lateral portion of the brow as a result of the compensatory contraction of the lateral fibers of the frontalis muscle. The result is the well-known Mephisto effect (Fig. 2).

The 5 traditional injection sites for treatment of the glabellar region. Doctors attempting to inject the corrugator supercilii muscle often inject the lower portion of the frontalis muscle instead, causing the medial portion of the brow to descend and the lateral portion of the brow to arch upward unnaturally, generating a Mephisto effect.

In some cases, we use a higher concentration of botulinum toxin in order to achieve greater precision and relax only the corrugator supercilii muscle. In our experience, this approach allows us to inject a smaller volume of liquid, thereby decreasing the likelihood of diffusion to unintended muscles (in this case, the frontalis).
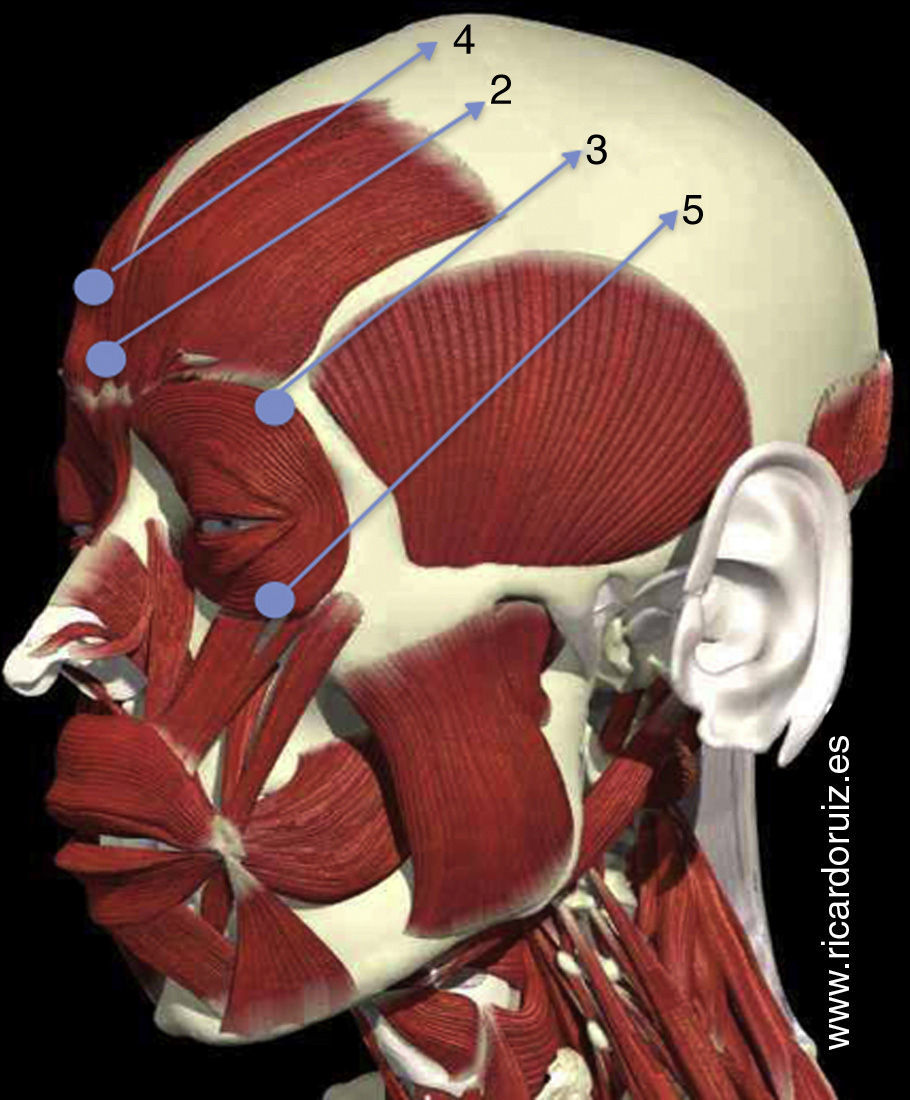
Always Injecting the Superior-Lateral Portion of the Orbicularis Oculi MuscleResult: Excessively Elevated EyebrowsInfiltration of botulinum toxin into the superior-lateral fibers of the orbicularis oculi muscle (Fig. 3) relaxes those fibers and lifts the lateral portion of the brow. The problem is that, in many patients, the position of the eyebrows moves upward with age as a result of the physiological contraction of the frontalis muscle.

Injection at point 2 can result in the Mephisto effect. Injection at point 3 lifts the lateral portion of the brow; in some patients, it may lift the brow excessively. Injection at point 4 can relax the frontalis muscle; in some patients, it can cause eyelid ptosis. Injection at point 5 can relax the orbicularis oculi muscle and exacerbate the undereye bags.
In one study,4 photographs were analyzed in order to compare eyebrow position in young patients and in patients 30 or 40 years older. Paradoxically, the study found that a physiological elevation of the eyebrows tends to occur with age in most patients. Therefore, for natural results, the superior-lateral fibers of the orbicularis oculi muscle should only be injected in patients in whom the lateral portion of the brow has descended.
Injecting the Frontalis Muscle in Patients Who Use it to Raise the EyelidsResult: Brow and/or Eyelid PtosisIn our experience, we have observed that many patients aged 65 years or older use the frontalis muscle to keep their eyes open. In these patients, relaxation of the frontalis muscle with botulinum toxin (Fig. 3) results in ptosis of the brows and/or eyelids. Therefore, in patients aged 65 years or older, the physician should examine the frontalis muscle and avoid injecting it if the patient uses it to open the eyes.
Injecting Too Low in the Crow's FeetResult: Exacerbation of Undereye BagsSome patients have undereye bags as a result of herniated fat or fluid retention. In either case, botulinum toxin injection can exacerbate these bags if the inferior fibers of the orbicularis oculi muscle are relaxed excessively. Therefore, in patients with a tendency to develop undereye bags, injection of the most inferior portion of the crow's feet should be avoided in order to preserve the tone of the corresponding region of the orbicularis oculi muscle.
Five Errors of OmissionFailure to Inject the Lower Third of the FaceResult: Less Effective Overall ResultWhen administering botulinum toxin injections, the physician should consider the patient's face as a whole, with the aim of relaxing the main depressor muscles in both the upper third—where the results are most gratifying—and the lower third. The problem is that undesired effects in the lower third of the face can lead to both cosmetic and functional deficiencies. It is therefore essential to use low doses in order to avoid complications.
In the lower third of the face, we can relax the platysma muscle at the jawline (a technique known as the “Nefertiti lift”),5 the depressor septi nasi muscle (in patients who have a plunging nasal tip when they smile),6 the depressor anguli oris muscle (to lift the corners of the mouth),7 the mentalis muscle (to relax the “pebbly” effect caused by the insertion of this muscle on the skin),8 etc.
The masseter muscle, which is used for chewing, is hypertrophied in some patients, causing both functional alterations (bruxism) and cosmetic alterations (square face). Injecting botulinum toxin into this muscle not only improves the symptoms of bruxism but also transforms a square face into a more oval shape.9,10 When injecting the masseter muscle, the location of the risorius muscle should be taken into account because diffusion of the toxin into this muscle can result in an asymmetrical smile.11
Failure to Inject Wrinkles Caused by Botulinum ToxinResult: “Unnatural” WrinklesWhen certain muscles are relaxed with botulinum toxin, the adjacent muscles increase in tone as they compensate for the inactivity of the treated muscles. This compensation has a desirable lifting effect, but it can also lead to new telltale wrinkles. The classic wrinkles caused by botulinum toxin—“bunny lines”—are caused by the contraction of the nasalis muscle (Fig. 4),12 but the contraction of fibers in the inferior portion of the orbicularis oculi muscle, in the frontalis muscle just above the eyebrows or at the hairline, etc., can also cause new wrinkles. These wrinkles should be corrected with botulinum toxin treatment.
Lack of Familiarity With Muscle Contraction PatternsResult: Unnatural Appearance
The appropriate injection sites vary from patient to patient. The “one size fits all” approach does not work in botulinum toxin treatment. Physicians should be familiar with the basic contraction patterns of the glabella,13–15 the forehead,16 and the crow's feet17 so that they can personalize the injection pattern for each patient, thereby achieving more natural results and using a smaller amount of botulinum toxin.
Failure to Differentiate Between Men's and Women's EyebrowsResult: Masculinization of Women's Appearance and Feminization of Men's AppearanceThe “seagull wing” is the classic eyebrow shape in women, whereas men's eyebrows are straighter and closer to the upper eyelids. The eyebrows can be shaped by relaxing the frontalis muscle, which lowers the brow at the injection site, or by relaxing the superior-lateral fibers of the orbicularis oculi muscle, which lifts the lateral portion of the brow. To lift the medial portion of the brow, botulinum toxin should be injected into the 3 depressor muscles in this area: the procerus, the corrugator supercilii, and the depressor supercilii.
Failure to Combine Botulinum Toxin with Other TreatmentsResult: Suboptimal ResultsBotulinum toxin is an excellent treatment for controlling certain expression lines and adjusting the position of certain facial features, including the brows, the nose, and the mouth. However, in the interest of achieving an excellent outcome, physicians should explain to patients that a prudent combination of botulinum toxin injection and other cosmetic treatments yields the best results.
One of the most important signs of facial aging is the loss of volume caused by changes in the fat compartments and bones of the face.18 In light of these changes, it is easy to see why the combination of botulinum toxin, dermal fillers, and collagen induction therapy—a “3-dimensional” approach—achieves the most natural results.
By combining this approach with fractional laser treatment, focused ultrasound treatment, and laser treatment of pigmented and vascular lesions, it is possible to safely and effectively correct the various signs of facial aging.19
Reflections on Botulinum ToxinIn order to achieve natural results with botulinum toxin, the physician should have exhaustive knowledge of the anatomy and functionality of the facial muscles. In our experience, cadaver anatomy courses and the treatment of patients with facial paralysis provide excellent opportunities to learn about the anatomy and functionality of the facial muscles; this knowledge can help physicians to optimize the cosmetic results of botulinum toxin treatment.
Many patients tell us that they do not recognize themselves in the mirror—that the face ages more quickly than the mind. They seek treatment in order to align their appearance with how they feel. Curiously, the transformations that our faces undergo with age mimic those which occur when we make an expression of sadness—in other words, the action of the depressor muscles is predominant.20 Botulinum toxin is an effective tool for relaxing the depressor muscles of the entire face, thereby reactively strengthening the levator muscles.
Facial rejuvenation treatment is currently based on a global 3-dimensional approach. However, there is also a fourth dimension: our expressions (in other words, the information transmitted by facial muscle movements). In order to communicate correctly, we must express our feelings through expressions. These expressions, in turn, influence the moods of the people around us. A patient recently told us that the atmosphere in her business and board meetings has improved greatly since she started receiving botulinum toxin injections. Indeed, the electromyographic activity of the zygomaticus major muscle—which controls the smile—has been shown to increase when we look at happy faces, while corrugator supercilii activity increases when we look at angry faces.20
Botulinum toxin also causes a very interesting feedback effect: our expressions depend on what we feel, but our feelings also depend on our expressions. Research has shown that patients who receive botulinum toxin injections are less likely to have depression or anxiety than patients who undergo other cosmetic techniques.21 Under normal conditions, emotion and expression are linked. Botulinum toxin breaks this link, raising an interesting question: If we cannot use facial expressions to express some of the emotions that we feel, do those emotions tend to disappear? This question has not yet been fully answered.
From conferences to textbooks, much has been said about the canon of beauty and how it should be applied to achieve the best cosmetic results. As Saint Thomas Aquinas wrote, “the senses delight in things duly proportioned.” However, we believe that dermatologists should not help their patients pursue ideal beauty at all costs; instead, we should simply try to help them feel better. Being beautiful is feeling beautiful. Research has shown that a smile creates a much better first impression than clothing or cosmetic surgery.22 The objective of cosmetic dermatology is to apply dermatological advances and a good doctor-patient emotional connection to increase people's quality of life. We must develop our sensitivity in order to be able to detect each patient's potential for beauty—that fourth dimension mentioned above—and use cosmetic dermatology to help them age gracefully and discreetly (Figs. 5–8).




The authors declare that they have no conflict of interest.
Please cite this article as: Ruiz-Rodriguez R, Martin-Gorgojo A. Diez errores a evitar en la inyección de toxina botulínica. Actas Dermosifiliogr. 2015;106:458–464.



